





Abstract
Two patients with the same model of single-coil active fix implantable defibrillator lead presented with evidence of lead malfunction, in one case with an abrupt rise in pacing impedance and threshold and in the other with evidence of over-sensing. In both cases, the chest radiograph showed separation of conductors in the defibrillation lead from the main body of the lead.
Failure of implantable cardioverter-defibrillator (ICD) leads can occur by several mechanisms including dislodgement, cardiac perforation, conductor failure, and insulation failure some of which may be attributed to lead design. 1
Case 1
A 43-year-old woman survived an out of hospital cardiac arrest for which no cause was identified. Investigations included coronary angiography which was normal. A St Jude Riata 1582 active fix single-coil defibrillator lead was passed via the left cephalic vein and connected to a St Jude Atlas-VR ICD. Routine follow-up was unremarkable with a stable pacing threshold of 0.75 V at 0.5 ms and pacing impedance of 450 Ω. At a routine follow-up 44 months post-implant, the pacing threshold had risen to 1.75 V at 0.5 ms and lead impedance to 1300 Ω.
A lateral chest radiograph showed separation of at least two of the conductors of the ICD lead proximal to the defibrillation coil in the right atrium ( Figures 1 and 2 , arrows). This was not evident on the posteroanterior radiograph.
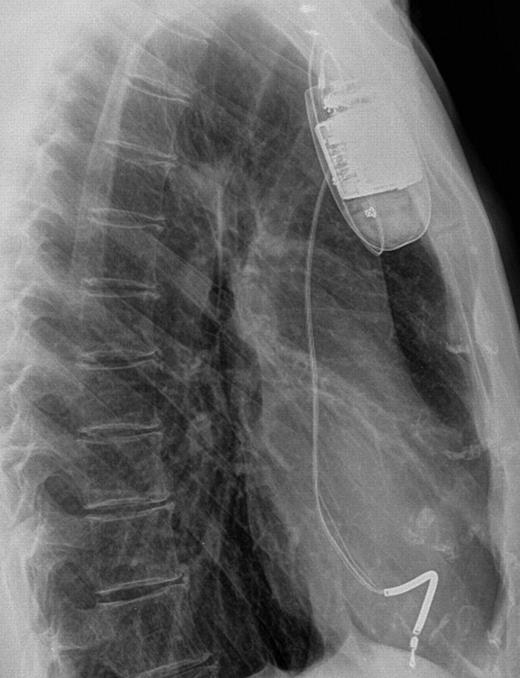
Lateral chest radiograph Case 1.
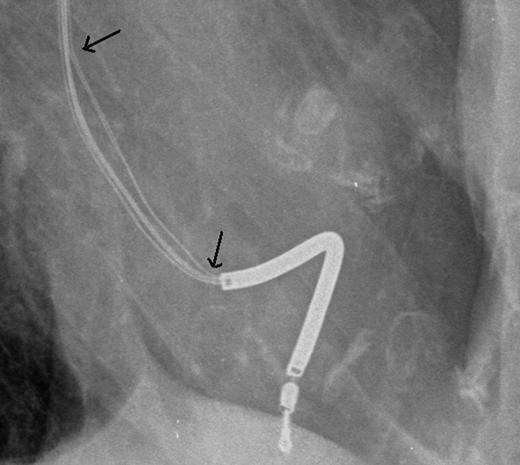
Lateral chest radiograph Case 1—detail.
Separation of conductor wire from the body of the lead has the potential to cause tissue damage. We evaluated the risk of lead extraction compared with the risk of retention in accordance with the HRS/AHA guidelines 2 and in view of the young age of the patient it was decided to extract the right ventricular lead. At transvenous lead extraction, it was not possible to pass a locking stylet beyond the proximal end of the defibrillation coil. Despite use of passive and active dissection sheaths, it proved impossible to free the lead and the locking stylet displaced. Extraction of the lead from the femoral route also failed. Considerable disruption of the lead had occurred during the procedure and we felt that the risks of lead abandonment were now considerable. The lead remnants were therefore extracted via thoracotomy.
Case 2
A 60-year-old woman presented with sustained VT and underwent CABG. VT was induced at subsequent electrophysiological testing. A St Jude Riata 1582 active fix single-coil defibrillator lead was passed via the left cephalic vein and connected to a St Jude Atlas-DR ICD. Routine follow-up was unremarkable with a stable pacing threshold of 0.75 V at 0.5 ms and pacing impedance of 400 Ω. At a routine follow-up, 63 months post-implant two short episodes of noise over-sensing, each triggering VF detection were noted. The patient had been using an electric drill and electrical interference was suspected. Lead impedance, shock circuit impedance, and pacing threshold were all stable. A posteroanterior chest radiograph was obtained but no abnormality was noted. After 6 weeks, during which the patient avoided further drilling, a device check revealed six further short episodes of noise triggering VF detection. Close scrutiny of the chest radiograph ( Figure 3 ) showed a pattern of conductor separation proximal to the defibrillation coil similar to Case 1. When compared with Case 1, the lifetime risk of lead retention was less in this older patient, and mindful of our previous experience in extracting a similar lead the patient was treated with placement of a new lead and abandonment of the failed lead.
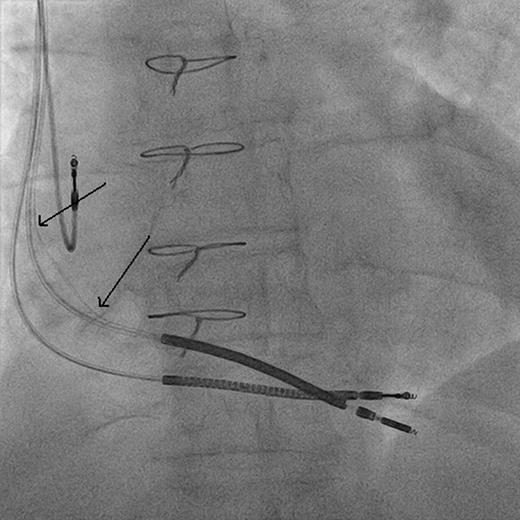
Posteroanterior chest radiograph Case 2 after new lead implanted.
Discussion
The St Jude Riata defibrillator lead family includes over 20 individual models. The Riata 1582 is a single-coil active fixation lead of multilumen construction with silicone insulation ( Figure 4 ). A central pacing coil connects to the lead's tip. Pairs of conductors are arranged in separate lumens in the outer part of the silicone insulation connecting to the proximal ring pacing electrode and the defibrillation coil electrode. The radiographs in each of these cases suggest that one pair of conductors has eroded through the lead insulation. The mechanism is unclear. In Case 1, the lead was so badly damaged by the extraction process that examination was unhelpful. In Case 2, the lead was left in situ . We have referred both cases to St Jude Medical and to the appropriate UK Regulatory Authority.
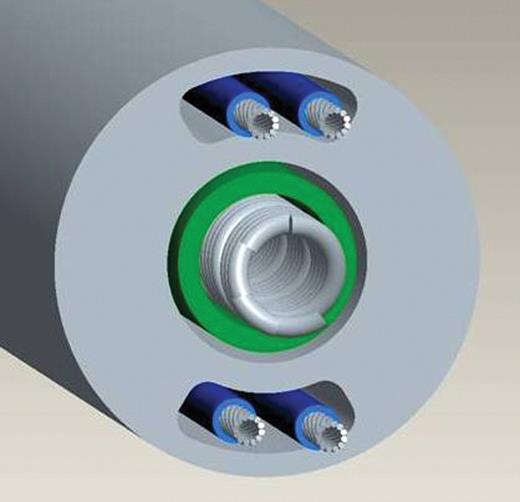
Schematic view of St Jude Riata single-coil lead, courtesy of St Jude Medical.
In a series of 7497 Riata leads followed for 22 months, insulation damage (nature unspecified) was reported in 0.13%. 3 Results were not presented by lead model and only 3% of leads in this series were model 1582. A multicentre analysis 4 of 15 387 Riata leads showed insulation damage in 0.21% but only 16% were followed up beyond 3 years and the data were not presented by model.
Out of 12 Riata 1582 leads implanted in this centre two have failed with radiographic evidence of conductor separation after 44 and 63 months. A single case of conductor separation in a Riata 1580 dual coil lead has also been reported 5 after an unspecified period of time. Whether this mode of failure will become more common as implant duration increases is unclear, but we would advise careful radiological inspection of any Riata lead with abnormal pacing or sensing parameters.
Conflict of interest: none declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}