





Abstract
We discuss a case of transvenous removal of endocardial leads in a patient with initial contraindication for such a procedure due to the size of the vegetation in his right atrium. Simultaneously, the patient's progressive general poor condition during the course of infective endocarditis prognosed that cardiosurgical intervention with the use of cardiopulmonary bypass would be unsuccessful. Using an innovative solution, that is placing the Dotter's basket in the right ventricular outlet as a protection against massive pulmonary embolism, the leads were removed. An asymptomatic pulmonary embolism caused by defragmented vegetation was revealed after the procedure.
Case report
In a 78-year-old patient, a 13-year-old pacing system consisting of the DDD pacemaker and two bipolar passive fixation leads (Biotronik TiR BP and TiJ BP) was present. The patient was pacing-dependent due to complete atrioventricular block. Current hospitalization was caused by multiorgan failure of several months duration during which infective endocarditis with 3.5 cm vegetation in right atrial chamber was revealed ( Figure 1 ). Both leads were blocked in the vegetation in the atrial base near the tricuspid valve. The only effective treatment of lead-dependent endocarditis should be a complete device removal with proper antibiotic therapy. 1 Lead removal from adhesions to the walls of the cardiovascular system is always connected with upsetting the vegetations. On the other hand, the risk of a major procedure with cardiopulmonary bypass to a patient in such a severe condition explained the disqualification from cardiosurgical intervention. 2 , 3 The transvenous lead removal procedure undertaken for life-saving indications with additional innovative protection against massive pulmonary embolism with the use of a Dotter's basket was decided upon. In the described case, the unfastened basket was considered to function as a sieve for displaced vegetation in case of its displacement in one big piece. In the case of the vegetation crumbling into smaller fragments, the Dotter's basket would not be useful to catch them as its openings are too big. In such a situation, though, the danger of massive pulmonary embolism would not be so big. The procedure was performed in a surgery room with anaesthetic and cardiosurgical back-up as well as monitoring of patient's life parameters, invasive blood pressure monitoring included.
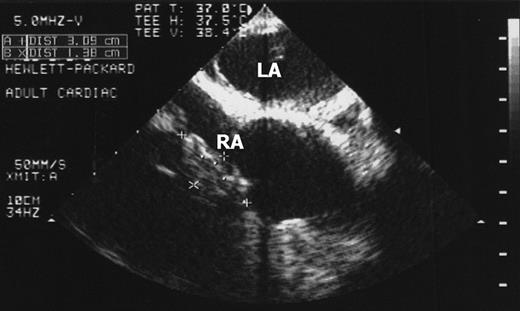
Illustration of a great vegetation connected with leads in the right atrium (RA) before the lead removal procedure: TEE picture (vegetation marked on the pictures).
By femoral venipuncture, the Byrd workstation was installed through which the Dotter's basket was introduced under the pulmonary valve. A temporary cardiac stimulation lead was also installed in the heart. The basket was unfastened for the whole 4 h long removal procedure. From upper access both leads were removed subsequently in compliance with the typical procedure using the Cook set. We used green and then white polypropylene Byrd dilators which proved to be enough to free the leads from the adhesions and the vegetation.
We did not use ‘locking stylet’ as introduction of the device in any diameter into the distal end of the lead was not possible. In order to make the lead more stiff for the removal procedure, we used a leader without anchoring function, which entered the lead as far as possible, that is, as far as the vegetation at the base of the right atrium. The higher number of leads and catheters in the right chambers of the heart increased the difficulty of the removal procedure. However, we assumed that the use of a subclavian approach for the removal of the lead and a femoral approach for the temporary stimulation lead and the Dotter's basket constituted the best solution.
The Dotter's basket stayed in the pulmonary outlet for two more hours after the procedure. No vegetation was found inside it. The echocardiographic (TTE and TEE) post-operative picture changed: a great vegetation disappeared and a smaller formation showed up balancing between the right atrium and the right ventricle. It was interpreted either as the ruptured papillary muscle or as the rest of the vegetation with no clinical significance. Computed tomography confirmed the disappearance of this great vegetation. Its crumbled pieces were found in the lobular and segmental branches of the right pulmonary artery ( Figure 2 ). The patient tolerated the intervention of lead removal well.
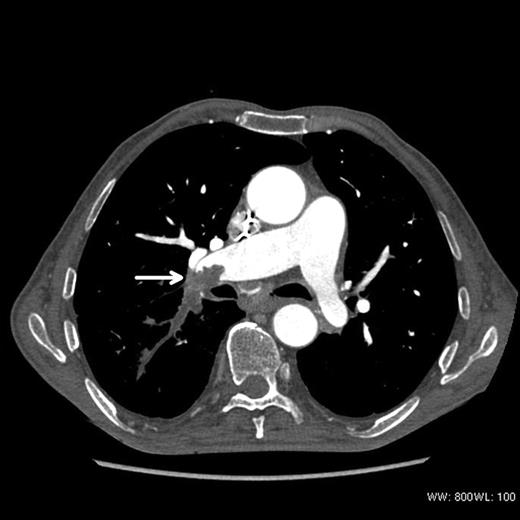
Computed tomography picture: defragmented vegetation obstructing lobular and segmental branches of the right pulmonary artery (arrow).
A new pacing system was implanted with a 15 day delay after the removal procedure with guided anti-staphylococcus antibiotic therapy being continued. At that time, the symptoms of lead dependent endocarditis subsided. We decided on implantation of a new stimulation system on the other side of the thorax despite the presence of a smaller formation in the heart because of the patient's dependence on the stimulation system and the presence of temporary stimulation protection. Blood culture test results were negative and other laboratory tests revealed no inflammatory state in the patient's body. He was discharged from hospital and has been under care of the outpatients clinic for 18 months.
Discussion
So far we have not found in medical literature any description of the procedure protecting the pulmonary bed against massive embolism. Single descriptions of transvenous lead removals with vegetations bigger than 2.5 cm in diameter are known. 4 , 5 Every time though, the doctors deciding on such a procedure risk the symptoms of massive pulmonary embolism which can occur due to the calibre of pulmonary arteries, into which the whole torn off vegetation can displace. The vegetation being crumbled during the lead removal procedure is less dangerous, because the fragments obstruct the pulmonary arteries of a smaller calibre. The use of a Dotter's basket in the outlet of the right ventricle allows for grasping this great vegetation in case it is torn off as a whole. The Dotter's basket, on the other hand, neither interferes with nor protects against flowing of small fragments of vegetation through the basket's openings. In the described case, the displacement of a crumbled vegetation to the pulmonary arteries with no clinical symptoms was confirmed.
The re-implantation of a new stimulation system was performed according to the principles for cardiovascular implantable electronic devices (CIED) replacement following infected removal (Class IIa, level of Evidence C): ‘It is reasonable to delay transvenous re-implantation of a new CIED system into patients with valvular or lead-associated vegetations for at least 14 days after CIED system removal’. 1
Conclusion
Very large vegetations may be removed transvenously. The protection of the right heart outlet track by a Dotter's basket during the removal of endocardial leads with large vegetations is feasible and does not obstruct dilatation. In the presented case, the protection was not helpful because the vegetation crumbled into pieces during the procedure.
Conflict of interest: none declared.

{kind=link}
{kind=link}