




Abstract
European Systematic Coronary Risk Assessment 2 for Older Persons (SCORE2-OP) model has shown modest performance when externally validated in selected cohorts. We aim to investigate its predictive performance and clinical utility for 10-year cardiovascular (CV) risk in an unbiased and representative cohort of older people of a low CV risk country. Furthermore, we explore whether other clinical or echocardiographic features could improve its performance.
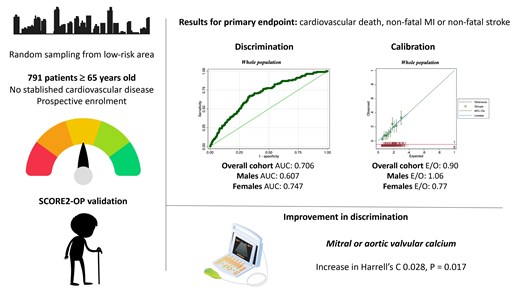
A cohort of randomly selected individuals ≥65 years from a primary care population of Barcelona without established CV disease included 791 patients (63.1% female, median age 76 years, median follow-up 11.8 years). The model’s performance yielded a Harrell’s C-statistic of 0.706 (95% confidence interval [CI] 0.659–0.753) for the primary endpoint (myocardial infarction, stroke, and CV mortality) and 0.692 (95% CI 0.649–0.734) for the secondary endpoint (primary endpoint plus heart failure hospitalization), with better discrimination in females. SCORE2-OP underestimated the risk of primary endpoint in women [expected/observed (E/O) = 0.77], slightly overestimated in men (E/O = 1.06), and systematically underestimated the risk of the secondary endpoint (E/O = 0.52). Decision curve analysis showed net clinical benefit across a 7.5–30% risk range for primary endpoint. Valvular calcification was the only variable that significantly improved 10-year SCORE2-OP risk performance for both primary and secondary endpoints, with a change in Harrell’s C of 0.028 (P = 0.017).
In a low CV risk country, SCORE2-OP showed notable discrimination and excellent calibration to predict 10-year CV risk, with better performance in females. Incorporating valvular calcification in a future revised score may enhance accuracy and reduce unnecessary treatments.
Lay Summary
The European Systematic Coronary Risk Evaluation 2 for Old Persons (SCORE2-OP) was developed to predict 10-year cardiovascular risk in the elderly, aiming to guide therapies whose effectiveness depends on the baseline risk profile. This research, involving 791 elderly individuals randomly selected from a low-risk Mediterranean area assessed the accuracy of the SCORE2-OP model in this population. The primary insights from the study are:
The SCORE2-OP model’s discrimination was reasonably good, but performed better in female than in male patients.
Despite good overall calibration, there is a tendency to underestimate the risk of cardiovascular events during follow-up, especially when heart failure admissions are considered.
Exploring alternative clinical and echocardiographic features may improve the model’s performance.



{kind=link}
Comments