





A relation to stress and stressful triggers is often, but not always, described in patients with Takotsubo syndrome. Few studies have focused on patients’ self-rated stress in combination with qualitative experiences of stress in Takotsubo syndrome.
The aim of this study was to describe stress before and after the onset of Takotsubo syndrome.
Twenty patients were recruited from five major hospitals in Stockholm, Sweden between December 2014 and November 2018. A mixed methods design was used containing the validated questionnaire, perceived stress scale (PSS-14) filled in at baseline and at a 6 and 12-month follow-up, respectively. Qualitative interviews were made at the 6-month follow-up.
Self-rated stress, measured by the perceived stress scale, showed stress levels above the cut-off value of 25, at the onset of Takotsubo syndrome (median 30.5). Stress had decreased significantly at the 12-month follow-up (median 20.5, P = 0.039) but remained high in one third of the patients. Qualitative interviews confirmed a high long-term stress and half of the patients had an acute stress trigger before the onset of Takotsubo syndrome. The qualitative interviews showed that the patients had reflected on and tried to find ways to deal with stress, but for many this was not successful.
Patients with Takotsubo syndrome reported long-term stress sometimes with an acute stress trigger before the onset of Takotsubo syndrome. Stress decreased over time but remained high for a considerable number of patients. Despite reflection over stress and attempts to deal with stress many were still affected after 6 months. New treatment options are needed for patients with Takotsubo syndrome.
Introduction
Takotsubo syndrome (TS) has been known since the early 1990s and was first reported from Japan by Sato and coworkers.1 It usually affects post-menopausal women and an apical ballooning shape of the left ventricle is most often seen and may lead to a severe dysfunction causing heart failure.2 A regression is usually seen within 3 weeks.1
Recent studies have shown that TS constitutes a significant proportion of patients with myocardial infarction with non-obstructive coronary arteries (MINOCA) which in turn affects up to 10% of all patients with myocardial infarction (MI).3,4 TS is more frequent in women3 and was previously described as a benign condition, but recent registry data indicate that the prognosis in terms of mortality is comparable to patients with coronary heart disease (CHD).5,6
Physical or emotional triggers, in some cases in combination, are seen in the majority (64–89%) of patients affected by TS.7,8 Triggers could be caused by psychological stress such as the sudden death of a relative, violence or natural disasters but also from physical stress due to diseases, that is, brain haemorrhage or sepsis.1 No stress or trigger was reported in 16–29% of the patients.7,8
Patients with TS report similar residual symptoms such as fatigue, breathlessness and chest pain, as patients with CHD 8 weeks after the acute event and long-term follow-up after one year indicate a negative impact on psychological wellbeing.9,10
One qualitative interview study conducted in hospital, or shortly after discharge, described long-term stressful circumstances among the participants that may have contributed to the onset of TS when being exposed to an acute trigger.11 Another study found that patients tried to handle their situation by avoiding stress after the acute event as they were afraid of the recurrence of TS.12 There is need for broader knowledge about stress in TS before and after onset, and quantitative, longitudinal data are lacking. Furthermore, patients own experiences are not fully explored in relation to self-rated stress, especially over time. The aim of this study was to explore further and describe self-reported stress as experienced by TS patients.
Methods
Study design
A mixed methods design was used consisting of questionnaires and narrative interviews regarding stress and coping abilities. The aim was to use a combination of quantitative and qualitative data results amplifying each other.13 Data were analysed separately but were finally integrated and discussed.
Patients
All patients in the present study had a diagnosis of TS according to Mayo Clinic diagnostic criteria including akinesia or dyskinesia in the left ventricle, absence of coronary disease, new electrocardiographic abnormalities and absence of the following conditions: head trauma or intracranial bleeding, pheochromocytoma, obstructive epicardial coronary artery disease (CAD), myocarditis and hypertrophic cardiomyopathy.14 The participants in the present study were recruited from the Stockholm Myocardial Infarction with Normal Coronaries-2 (SMINC-2) study, the design of which is published elsewhere.15 Patients in SMINC-2 were recruited from five hospitals in the Stockholm area during hospital admission and received follow-up at 6 and 12 months, respectively. Twenty patients were recruited consecutively between December 2015 and June 2018 for the interviews. The patients were contacted by a telephone before the planned 6 months visit for participation in the interview and the informed consent was sent by mail. All suitable patients consented to participation, which resulted in 20 interviews. The researchers had no care relationship with any of the patients.
The perceived stress scale (PSS-14)
PSS-14 is a self-reported questionnaire measuring levels of stress and coping. The participants estimate how and to what degree they experience their life unpredictable, uncontrollably and overloaded in the past month.16 PSS-14 was measured at baseline (onset of TS) and at 6 and 12 months. PSS-14 contains 14 items and every item has five different options, between zero (never) and four (very often). The lowest possible total score is zero and the highest is 56. High scores indicate more stress-related emotions and thoughts. The cut-off score for increased levels of stress is 25 or higher on the total scale.16 PSS-14 can be divided into two subscales in which seven of the items belong to factor 1, measuring stress, while the other seven items belong to factor 2, measuring coping ability.17 The Swedish version of PSS-14 has been shown to be valid in patients with or without known stress-related conditions.18 The questionnaires were processed with the statistical package for the social sciences (SPSS) software, version 23.19 The median and interquartile range (IQR) was used in box plots to show the values of PSS-14. Friedman’s test was used to compare PSS-14 at baseline, 6 and 12 months, respectively.
Qualitative interviews
An interview guide was developed with semistructured questions. The patients were encouraged to speak freely about their experience of stress, before, during and after the onset of TS. The interview questions were: ‘Can you describe how you felt the time before onset of TS?’ ‘Do you have any stress experiences in life?’ ‘Did something special occur just before or associated to onset of TS?’ ‘Could you describe how you felt the time after?’ ‘Could you describe if you have done any changes to reduce stress?’
Three of the authors (RS, CB and PL) performed the interviews at a face-to-face meeting in a private room at the hospital. The interviews lasted between 20 and 55 minutes. All interviews were recorded and transcribed verbatim by one author who did not perform that particular interview.
The interviews were analysed with content analysis according to Graneheim and Lundman.20 To obtain the sense of the whole meaning, the 20 interviews were read several times. Meaning units that suited the aim were marked and condensed to shorter passages. They were then added together in codes and classified into categories and subcategories to abstract the text further from the interviews. Finally, a theme emerged as the result from the interviews. The analyses were made separately by the first and second author (RS, CB) and discussed between the two researchers. The results were then discussed with the last author (PL) until consensus was reached.
Ethical considerations
The study was approved by the regional ethical review board, Stockholm, Sweden (Dnr. 2014/131-31/1 and 2015/2117-32) and conformed to the principles of the Declaration of Helsinki.21 Written informed consent was obtained and patients could withdraw their consent at any time without giving any reason.
Results
All 20 patients fulfilled the Mayo Clinic diagnostic criteria for TS. Baseline characteristics are presented in Table 1.
Baseline characteristics for patients with Takotsubo syndrome.
| Baseline characteristics | Number of subjects (n = 20) |
|---|---|
| Mean age, SD, years (range) | 59 ± 8 (47–70) |
| Gender (female) | 18 |
| Married/cohabiting | 15 |
| Children | 19 |
| Employed | 15 |
| Retired | 5 |
| Heredity, CAD (<65 years) | 9 |
| Smoker | 3 |
| Never smoked | 6 |
| Former smoker | 10 |
| Hypertension (treatment) | 6 |
| Depression | 1 |
| Post menopause | 15 |
| Baseline characteristics | Number of subjects (n = 20) |
|---|---|
| Mean age, SD, years (range) | 59 ± 8 (47–70) |
| Gender (female) | 18 |
| Married/cohabiting | 15 |
| Children | 19 |
| Employed | 15 |
| Retired | 5 |
| Heredity, CAD (<65 years) | 9 |
| Smoker | 3 |
| Never smoked | 6 |
| Former smoker | 10 |
| Hypertension (treatment) | 6 |
| Depression | 1 |
| Post menopause | 15 |
Values are mean ± SD, range and numbers.
CAD: coronary artery disease.
Baseline characteristics for patients with Takotsubo syndrome.
| Baseline characteristics | Number of subjects (n = 20) |
|---|---|
| Mean age, SD, years (range) | 59 ± 8 (47–70) |
| Gender (female) | 18 |
| Married/cohabiting | 15 |
| Children | 19 |
| Employed | 15 |
| Retired | 5 |
| Heredity, CAD (<65 years) | 9 |
| Smoker | 3 |
| Never smoked | 6 |
| Former smoker | 10 |
| Hypertension (treatment) | 6 |
| Depression | 1 |
| Post menopause | 15 |
| Baseline characteristics | Number of subjects (n = 20) |
|---|---|
| Mean age, SD, years (range) | 59 ± 8 (47–70) |
| Gender (female) | 18 |
| Married/cohabiting | 15 |
| Children | 19 |
| Employed | 15 |
| Retired | 5 |
| Heredity, CAD (<65 years) | 9 |
| Smoker | 3 |
| Never smoked | 6 |
| Former smoker | 10 |
| Hypertension (treatment) | 6 |
| Depression | 1 |
| Post menopause | 15 |
Values are mean ± SD, range and numbers.
CAD: coronary artery disease.
None of the patients were on full time sick leave, but more than half were still on part-time sick leave 6 months after the onset of TS.
Results of PSS-14
Eighteen subjects filled in PSS-14 at baseline, 20 at 6 months, and 18 at the 12-month follow-up, respectively. The median value of PSS-14 at baseline was 30.5 (range between 8 and 46) and 12 of 18 patients scored 25 or higher. At 6 months the median score was 20.5 (range between 8 and 39), eight of 20 scored 25 or higher. At the 12-month follow-up the median value was 22.5 (range between 6 and 43). Eight of 18 scored 25 or higher. The total value of PSS-14 showed significantly greater stress at baseline compared to the 6 and 12-month follow-ups (P = 0.039). The scores of the subscale measuring stress (factor 1) were 16.7 at baseline, 13.0 at 6 months and 14.0 at 12-month follow-up. The scores for the subscale coping ability (factor 2) were 11.8 at baseline, 10.0 at 6 months and 9.9 at 12-month follow-up. The changes in scores for stress (factor 1) and coping (factor 2) were not statistically significant (P = 0.137 and 0.081, respectively) (see Figure 1).
Results of interview
The main result of the interviews conducted at the 6-month follow-up was the theme: ‘drained resources resulting in lack of balance’. The theme emerged from the four categories: ‘powerlessness’, ‘suppressed emotions’, ‘to be capable’ and ‘coping with stress’. An overview of the result, including subcategories, is presented in Figure 2.
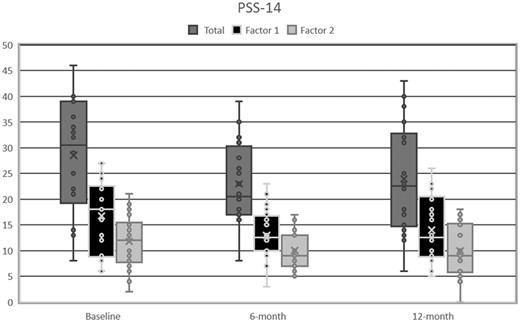
The perceived stress scale (PSS-14) total scale at baseline, 6 and 12 months and factors 1 (stress) and 2 (coping) at baseline, 6 and 12 months. Median values and interquartile ranges (IQRs) are given in box plots. P values for change over time (Friedman’s test): total scale P=0.039, factor 1 P=0.137, factor 2 P=0.081.
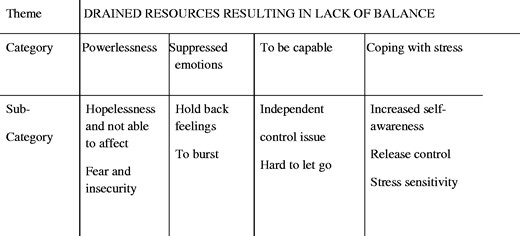
The results from the qualitative interviews presented as Theme, Categories and Sub-Categories.
Drained resources resulting in lack of balance
The theme ‘drained resources resulting in lack of balance’ contained experiences of long-term stress through life. To be able to handle a stressful situation, the patient had to restrain their feelings to keep things together. A common trait of character among the patients was to be competent and take a key role in every situation. When things got out of hand and the situation became unsustainable, they lost control and were not able to find a way out. All patients ended up at the emergency department with chest pain like MI, and half of them in connection with a strong emotional reaction. In the interviews it was expressed that patients had reflected over their situation after the onset of TS and had tried to change their behaviour. Still many described impaired stress resistance.
Powerlessness
Patients described long-term stress for years to decades. They described burdensome life events that had affected them throughout life. It could be life situations that were difficult to affect. The subcategory ‘not be able to affect’ contained descriptions of children going through troublesome periods, for example, drug abuse, beings bullied and having depression as exemplified by this statement, ‘The stress hit me like a bomb … one daughter had a breakdown and felt mentally ill without my knowledge … then everything fell’. Patients told about children with neuropsychiatric diseases and how they often had to fight for the children’s concern and wellbeing which ended up in several meetings at school and with social authorities. During periods, some patients had to set everything aside to focus only on their children. There were also worries about relatives who suffered from severe illnesses. Patients expressed situations going out of hand with a feeling of having no way out resulting in hopelessness. Within the subcategory of ‘fear and insecurity’ some patients mentioned parents that never encouraged them and how they had a feeling of not being good enough during childhood. Even threats and violence could appear. Parents could also be absent from home leaving responsibility to them at a young age. One patient expressed severe emotional pressure from the partner with both physical and psychological violence for a long time exemplified by this quote, ‘Felt a fearful pressure, never knowing the state of my partner when I came home’. To not be able to affect life circumstances led to a sense of powerlessness.
Suppressed emotions
In general, the patients had to suppress their own emotions to cope with stressful life events. Within the subcategory of ‘holding back feelings’ patients told how they were used to cover things up and not expose their emotions. Some had not been angry for decades and instead turned these feelings inward. Descriptions of struggling for a long period of time despite a total loss of energy arose. Some told it was the only option, because the most important thing was their children’s wellbeing. To be positive was an approach to set their own feelings apart to make life work altogether as stated by one patient. ‘Unfortunately, I put a happy face on, always happy no worries, it will work out’.
Severe stress-filled events had occurred for the patients and these were often close to the onset of TS. This was common in the subcategory ‘to burst’. Patients expressed things that became too much to handle as one patient said. ‘I remember that I cried a lot and it was a lot of crap that came out … it was a lot of unmet needs, I think. It was impossible to suppress the emotions and sorrows, everything just burst out’. Half of the patients expressed a severe emotional reaction just before the acute onset.
To be capable
To experience themselves as capable and being a doer was described among the patients. In the subcategory of ‘independence’ patients expressed how they liked to work hard and independently as told by one patient, ‘I think I’m used to feel pretty strong ever since youth and have never asked anybody for help, to be self-sufficient no matter what’.
To set one’s heart and soul into their work and not leaving anything incomplete was described among the patients in the subcategory of ‘control issue’. Being high-performance, competitive and ambitious and to be structured in every detail led to stressful situations. This became obvious when things turned out different from the original plan as told by one patient, ‘When I’m not able to affect things, it gets really tough’.
Even little worries were hard to let go even though others thought they were less important. Patients remembered memories of insecurity from their childhood. To take great responsibility for insufficient parents in situations of abuse and mental illness was believed to result in a control need that followed them through life. Patients described how they had a strong need for confirmation and it was important to be a person that others could rely on both in private life and at work.
Coping with stress
The patients had in different ways tried to cope with their stress after the TS event. There were patients that had been offered professional support from healthcare professionals. They experienced the support given as positive and helpful to find new coping strategies to reduce their stress. In the subcategory ‘increased self-awareness’ patients struggled to change their behaviours and their way of thinking to listen better to the signals from their body as expressed by this patient, ‘I have had enough; my body cannot take it anymore. I really try to put myself as the priority, when it is possible’.
Within the subcategory ‘to release the control’ patients described the importance of being aware of their own feelings. To learn how to set limits at work but also in private life as told by one patient, ‘Now I had a legal reason not always be available to solve everything, as I used to do before’.
There were descriptions of negative impact on life due to limited resources to handle different impressions. More than half of the patients described in the subcategory of ‘stress sensitivity’ that their stress sensitivity had increased after the onset of TS. They experienced themselves as more vulnerable after the TS event. Consequences could be sleeping disorder, memory loss, loss of concentration, reading difficulties and sound sensibility and for some patients this could lead to avoiding social events. One patient expressed that the words did not fasten, it just rebounded. ‘The brain felt overloaded, I cannot take in more information’. Most patients stated how their own resources were not sufficient to deal with stressful life events.
Discussion
The results of this first mixed methods study on stress in TS showed high levels of stress before and at the onset of TS. Self-rated stress decreased after 6 months and remained stable at the 12-month follow-up as measured by the PSS-14. When interview data were added after 6 months they confirmed long-term stress among the patients and the theme ‘drained resources resulting in lack of balance’ emerged. Half of the patients described an acute emotional stressful incident before the onset of TS. The findings are in line with several other studies that have shown how a stressful emotional or physical trigger are typical for TS but are not always present.8,22 After 6 months when the patients have had time to reflect over their situation the majority of them expressed higher stress sensitivity than before the onset of TS.
Two-thirds of the patients with TS scored 25 or higher on PSS-14 that is the cut-off value for increased stress. The median value of 30.5 is comparable to women treated for stress-related disorders (mean 29.6), and the same study contained a healthy control group with a lower score (mean 24.8).18 A similar decrease in self-rated stress over time as seen in the present study was also seen among young and middle-aged patients after MI.23 Yet another study comparing patients with MINOCA and MI showed a median value above the cut-off of 25 which dropped in both groups over time after the acute event.24 Patients with another severe condition, that is, gastrointestinal cancer, reported lower scores than patients with TS at the time of diagnosis.25 The decrease of PSS-14 seen in the present study was most evident during the first 6 months after the acute event and could be part of the natural recovery process. Still, more than one third scored 25 or above after 12 months. PSS-14 can be divided into two subscales measuring stress, factor 1, and coping, factor 2.17,18 None of them changed significantly over time but a trend (P = 0.08) towards better coping was seen. This was also mentioned in some of the interviews in which patients told how they had reflected over their situation and in some cases changed habits. However, most patients felt more vulnerable after 6 months than before the onset of TS, and that coping strategies were used by many patients but that their own resources were not sufficient to handle stressful situations indicating a need for support and structured follow-up. The complexity of this task is shown by the diverging results by Kastaun et al.,26 who found that TS patients had as good coping strategies as patients with MI and healthy controls, whereas Hefner and Csef27 concluded that patients with TS used positive coping strategies less often than healthy individuals.
In the interviews the theme ‘drained resources resulting in lack of balance’ emerged from the four categories ‘powerlessness’, ‘suppressed emotions’, ‘to be capable’ and ‘coping with stres’. Almost all patients described long-term stress that had affected them through life. It could be unhealthy relationships and concerns about children’s wellbeing. This is in line with other studies indicating a connection between a burdensome life situation and TS.11,12,28 In a sample of 45 patients with TS, 44% had chronic psychological stress prior to the onset of TS.29 Powerlessness and high demands were explained by Perski and Osika30 as a threat that often led to stress reactions in accordance with this paper. Patients in our study described difficulties influencing their own situation, which led to a sense of powerlessness. They also told how they suppressed their emotions, and how their own needs had to be set aside.
Our result showed that TS patients had a large emotional commitment in care for relatives and in their professional work. They also reported high demands, responsibilities and described themselves as capable persons, similar to the findings in other studies.11,12 Individuals normally show a wide variety of receptiveness and resistance to stress. Those who have a good stress response manage to deal with stressful situations, while those who have difficulties dealing with stressful events may suffer from stress-related conditions.31
Many had reflected about themselves and their own needs and desires after the acute TS event. TS patients expressed that it was time to make changes in daily life and prioritise themselves, and to find new strategies to cope better with their stress. Some were offered support from healthcare professionals while others tried on their own, sometimes with support from relatives, to change behaviours. Patients with TS were not invited to education and cardiac rehabilitation that they potentially could benefit from because they lacked CAD.32 Granitto et al.33 concluded that it is important with support from healthcare professionals to explain the connection between TS and stress and to identify anxiety and stress to be able to explore different ways of adopting coping strategies. Support and follow-up are of great importance as it is not only TS patients’ own behaviour that has to be changed, but the need to meet the demands from others. It is therefore important to offer this group a routine follow-up including individual support. Stress with a negative impact on life may occur when demands are high, and the resources are drained. This was obvious in the present study and the theme, ‘drained resources resulting in lack of balance’ discloses the feelings of patients with TS. As power and control are important protectors against stress it is of great importance to learn to recognise signals and patterns in stress and the potential to change behaviour when a threatful situation occurs.30 In addition to routine follow-up, internet-based cognitive behaviour therapy may be an option in patients with TS as it has been tested successfully in cardiac patients regarding prognosis.34,35 Future research on patients with TS should focus on characterising self-rated stress. Randomised studies on interventions to reduce stress and thus improve quality of life are needed.
Our study has limitations. The sample size of 20 patients resulted in a small number of questionnaires thus making it difficult to generalise the results to other settings. PSS-14 measures perceived stress during the past month. It may be difficult for patients to consider in relation to an acute cardiac event such as TS. A strength in comparison with other studies11,12 is that all 20 interviews were made at the same time 6 months after the onset of TS. The patients then have had time to reflect on their situation and were not affected by being hospitalised with acute cardiac symptoms. However, recall bias cannot be ruled out, but 20 questionnaires with a validated questionnaire (PSS-14) reinforced each other resulting in a deeper understanding of experience of stress in TS patients.
Conclusions
Patients with TS reported long-term stress and half of them an acute stress trigger before the onset of TS. Stress decreased over time but remained high for a considerable number of patients. Despite reflection over stress and attempts to deal with stress many were still affected after 6 months.
Implications for practice
• High stress is common in patients with Takotsubo syndrome. • Structured follow-up is needed for these patients. • New treatments should be developed and tested in trials.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Riksförbundet Hjärt-Lung.
References
Author notes
The first two authors are joint first authors

{kind=link}
{kind=link}
Comments