Abstract
The wide availability of effective drugs in reducing cardiovascular events together with the use of myocardial revascularization has greatly improved the prognosis of patients with coronary artery disease. The combination of antithrombotic drugs to be administered before the knowledge of the coronary anatomy and before the consequent therapeutic strategies, can allow to anticipate optimal treatment, but can also expose the patients at risk of bleeding that, especially in acute coronary syndromes, can significantly weigh on their prognosis, even more than the expected theoretical benefit. In non ST-elevation acute coronary syndromes patients in particular, we propose a ‘selective pre-treatment’ with P2Y12 inhibitors, based on the ischaemic risk, on the bleeding risk and on the time scheduled for the execution of coronary angiography. Much of the problems concerning this issue would be resolved by an early access to coronary angiography, particularly for patients at higher ischaemic and bleeding risk.
Revised by Antonio Francesco Amico. Matteo Cassin, Emilio Di Lorenzo, Luciano Moretti, Alessandro Parolari, Emanuela Pccaluga, Paolo Rubartelli
Consensus Document Approval Faculty in appendix
Introduction
The great efficacy in the treatment of acute coronary syndromes (ACS) and coronary disease in general, can be attributed to the diffusion of myocardial revascularization by both percutaneous coronary intervention (PCI) and coronary artery bypass graft (CABG), and to the availability of antithrombotic drugs that effectively reduce ischaemic complications. It is a widespread practice to administer antiplatelet and/or anticoagulant therapy before performing coronary angiography (a strategy known as ‘pre-treatment’) in order to prevent ischaemic events before a revascularization procedure and to reduce peri-procedural infarction in case of PCI. Pre-treatment may however, expose the patient to haemorrhagic complications without providing any benefit in case of low ischaemic risk, or require its rapid discontinuation in case of surgical revascularization. Pre-treatment may furthermore provide very different theoretical benefits according to the patient's clinical conditions, as they could be greater in acute syndromes, where the instability of the atherosclerotic plaque and thrombosis prevail.
The choice of the drugs to be administered before invasive intervention is made more complex since the last European Society of Cardiology (ESC) guidelines on non ST-segment elevation (NSTE) ACS1 state that patients with ischaemia-induced troponin elevation, who are defined as being at high risk, should be referred for a coronary angiography within 24 h; something that actually occurs in a minority of patients.
This consensus document, which was drawn up by experts from the leading Italian societies of cardiology, aims to provide an instrument to guide the choice of treatments as well-suited as possible to the clinical condition of patients candidates to myocardial revascularization.
Suggested options are summarized in tables reported at the end of every chapter. The weight of the recommendations is shown on a coloured scale: the recommended treatment appears in green; the optional treatment for which a favourable opinion prevails appears in yellow; a treatment that is possible, but only in selected cases is in orange whereas contraindicated treatments are in the red column.
ST-segment elevation acute coronary syndrome
Antiplatelet drugs
Oral antiplatelet agents
Pre-treatment with aspirin is recommended in all ST-segment elevation acute coronary syndrome (STE ACS) patients’ candidates for PCI, but no specific data are available in the literature.2
In patients with STE ACS, angioplasty is usually performed within a few hours or minutes, making difficult to effectively inhibit platelets hyperactivity by oral agents, given their metabolism and bioavailability.
Pre-treatment with clopidogrel in the patient subgroup of the CLARITY-TIMI 28 study3 undergoing PCI reduced the incidence of major adverse cardiovascular events (MACE) without a significant increase in bleeding.4 However, PCI was performed hours after thrombolysis. Successively, two studies on primary PCI did not reveal any significant benefit from pre-treatment.5,6 Lastly, the ACTION meta-analysis showed a significant reduction in MACE with clopidogrel pre-treatment without increase in major bleeds.7
The superiority of prasugrel and ticagrelor compared with clopidogrel in reducing MACE in ACS patients was demonstrated by both TRITON TIMI-388 and PLATO studies.9 The new antiplatelet drugs were more effective than clopidogrel even in the STE ACS subgroup10,11; however, very few data are available on pre-treatment and in patients undergoing primary PCI.
The only randomized trial on pre-hospital treatment with a P2Y12 inhibitor is the ATLANTIC study,12 in which no difference was observed in pre- and post-PCI reperfusion markers by ticagrelor pre-treatment, compared with its cath lab administration; the mean time difference between the two strategies was a mere 31 min. Pre-treatment with ticagrelor did not reduce MACE, but without an increased risk of bleeding.
Despite the lack of evidence from randomized trials, early administration of a P2Y12 inhibitor, preferably prasugrel or ticagrelor, would seem advisable, even in the ambulance if allowed by local organization, especially if the patient transport time exceeds 30 min. The administration of clopidogrel must be reserved for cases in which prasugrel and ticagrelor are contraindicated or not available.2
Glycoprotein IIb/IIIa inhibitors
Glycoprotein IIb/IIIa inhibitors (GPI) have been used in STE ACS to obtain an effective anti-platelet action during angioplasty. A meta-regression performed by De Luca G. et al.13 showed a significant relationship between the patient risk profile and the reduction in mortality in patients pre-treated with GPI. However, many of the studies included were conducted without systematic use of GPI.
In patients pre-treated with clopidogrel, the HORIZONS-AMI trial14 showed the superiority of pre-treatment with bivalirudin over unfractionated heparin combined with abciximab. In patients pre-treated with a loading dose of clopidogrel, the BRAVE-3 study15 did not show any advantage from the administration of abciximab on the amount of myocardial necrosis.
These data suggest that routine up-stream use of a GPI does not yield benefits in terms of outcome, whilst increasing the risk of bleeding,16 and is therefore generally not indicated. It may be considered in patients with a high thrombotic risk and low haemorrhagic risk, for whom PCI is delayed due to longer transfer time.12,17
Anticoagulants
Although there are no specific data on the up-stream administration of unfractioned heparin (UFH) in patients with STE ACS scheduled for primary PCI, its use would appear to be reasonable.2
Enoxaparin is a potential option; however, in the ATOLL study18 it doesn’t demonstrate to be superior to UFH in reducing ischaemic and haemorrhagic events.
Bivalirudin would appear to be preferable in patients at high haemorrhagic risk, for its efficacy similar to UFH associated with GPI but with a lower incidence of bleeding; its use was associated with a reduction in total and cardiovascular mortality, but increased the incidence of intra-stent thrombosis.19,20 It should be pointed out that bivalirudin favourable results have not always been confirmed.21,22
It is not therefore possible to pinpoint the best anticoagulant treatment, but the choice should be taken depending on the characteristics of the individual patient. In cases of low haemorrhagic risk and low thrombotic burden, UFH or enoxaparin are reasonable options. In those patients treated with a combination of UFH and GPI, which guarantees excellent antithrombotic efficacy but increases haemorrhagic risk, it is fundamental not to overdose heparin and to privilege radial access. Bivalirudin, on the other hand, should be preferred in patients with a higher haemorrhagic risk or in those with delayed presentation, in whom GPI are less effective.
Anticoagulant therapy should be discontinued after PCI, except in patients in whom it has a specific indication or for the prophylaxis of venous thromboembolism.
There are no randomized studies available on parenteral anticoagulant therapy in patients on oral anticoagulant therapy (OAT) to be treated with primary PCI, only expert opinions.23,24 Regardless of whether the patient is on treatment with a vitamin K antagonist or with a new oral anticoagulant (NOA), it is nevertheless required to administer an additional dose of i.v. anticoagulant, like reduced-dose UFH or bivalirudin, which has a lower bleeding risk.
Anti-ischaemic drugs
Beta-blockers
Beta-blockers have shown to reduce mortality in the acute phase of STE ACS in the pre-thrombolytic age25,26; however, the evidence of a benefit in primary PCI treated patients is inconsistent. Early use of high doses is associated with increased mortality,27 particularly in patients at risk of developing cardiogenic shock.28
Calcium channel-blockers
Verapamil and diltiazem own an efficacy similar to that of beta-blockers in reducing heart rate and symptoms; however, in the acute phases of STE ACS they could be potentially harmful and should therefore not be used.29
Nitrates
Routine administration of nitrates in STE ACS is generally not recommended2; their usefulness has been however, acknowledged in patients with hypertension or heart failure.
Statins
In patients with STE ACS high-dose statins should be administered early and continued in the long term, with a target low density lipoprotein cholesterol level (C-LDL) below 70 mg/dL.2 This treatment is recommended regardless of reperfusion therapy.
Statins could have ‘pleiotropic effects’ on vessel walls, with anti-inflammatory, antioxidant, and antithrombotic properties that could improve endothelial function and stabilize the atherosclerotic disease.30 They have been used in primary PCI in an attempt to reduce the extent of myocardial damage and favour optimal reperfusion.31–35 High doses of high efficacy statins (atorvastatin 80 mg and rosuvastatin 40 mg), administered immediately before primary PCI could improve both epicardial (TIMI flow and TIMI frame count) and myocardial reperfusion (TIMI myocardial perfusion grade or myocardial blush grade), and could reduce the incidence of no-reflow and the levels of myocardial damage markers.
Studies on this topic are too small to demonstrate a definite effect of pre-treatment; however, given the lack of significant side effects in the acute phase, it would seem appropriate to suggest their early administration.
In Italy statin prescription is ruled by circular no. 13 issued by the Italian Medicines Agency (AIFA),36 which identifies high-dose atorvastatin (≥40 mg/day) as the first treatment option in patients with ACS and/or undergoing myocardial revascularization.
Suggested treatment options for STE ACS patients are summarized in Table 1.
Table 1ST-segment elevation acute coronary syndromes pre-treatment
Table 1ST-segment elevation acute coronary syndromes pre-treatment
Non ST-segment elevation acute coronary syndrome
Antiplatelet drugs
Oral antiplatelet agents
The ESC 2011 guidelines on NSTE ACS37 recommended the administration of aspirin and P2Y12 inhibitors ‘as soon as possible’, whereas the 2015 edition suggests that this treatment should be administered timely from the time of diagnosis, without however providing specific indications about when, and recommending haemorrhagic risk stratification.1 Invasive strategy should be adopted:
immediately (within 2 h of diagnosis) for patients with haemodynamic or electric instability, or another very high risk criterion;
early (with 24 h of diagnosis) in patients with at least one high risk criterion, including troponin elevation;
electively (within 72 h of diagnosis) in patients with at least one intermediate ischaemic risk criterion.
Aspirin
Aspirin has demonstrated to be effective in patients with unstable angina38; the incidence of myocardial infarction or death was reduced in four trials in the pre-PCI era.39–42 A meta-analysis of these studies showed a significant reduction at 2 years in the MACE rate.43 However, there are no specific data available on the administration before an invasive strategy.
Clopidogrel
The pre-treatment strategy comes from the results of the PCI-CURE trial,44 in which a 30% reduction in the primary endpoint of death, infarction or stroke was seen in patients pre-treated with clopidogrel; however, this sub-group represents only about 20% of the whole CURE trial population, and the average time interval between pre-treatment and PCI was 10 days, which is far longer than nowadays.
Prasugrel
The only randomized trial on pre-treatment with a P2Y12 inhibitor in patients with NSTE ACS is the ACCOAST study,45 in which patients intended for an invasive approach were randomized to receive pre-treatment with an oral loading dose of 30 mg of prasugrel followed by a further oral 30 mg load at the time of PCI, or the administration of 60 mg of prasugrel in the cath lab. The mean duration of pre-treatment was 4.3 h. At 7 days no reduction was observed in the occurrence of the primary endpoint, while major bleeds where significantly increased in the pre-treatment arm. Pre-treatment with prasugrel in patients with NSTE ACS is therefore not recommended.1
Ticagrelor
In the NSTE ACS patient subgroup of the PLATO study, the primary composite efficacy endpoint was significantly reduced by ticagrelor compared with clopidogrel;46 however, results in patients actually pre-treated are not available.
Intravenous antiplatelet agents
Cangrelor
Cangrelor is a direct reversible inhibitor of P2Y12 receptor, that has been compared with clopidogrel in patients undergoing PCI,47–49 most of whom affected by ACS. A meta-analysis of these trials showed that the infusion of cangrelor reduced the relative risk of the composite endpoint (peri-procedural death, myocardial infarction, ischaemia-guided revascularization and intra-stent thrombosis), determining also an increase in minor and major bleeds, but not in the need for transfusions.50
European Society of Cardiology guidelines suggest considering pre-treatment with cangrelor in patients who are not treated with a P2Y12 inhibitor.1 Cangrelor, which has been approved by the European Medicines Agency, is currently not available in Italy.
Glycoprotein IIb/IIIa inhibitors
Up-stream use of GPI in patients with NSTE ACS has been studied in two trials. In the ACUITY,51 the deferred GPI administration strategy compared with the up-stream use led to a significant reduction at 30 days in major bleedings not related to CABG, without any difference in the primary efficacy endpoint. The EARLY-ACS study52 did not reveal any significant reduction in the primary endpoint occurrence in the arm pre-treated with eptifibatide compared with the optional use arm, but showed a significant increase in major bleeds. Lastly, a meta-analysis indicated that GPI pre-treatment did not reduce mortality or myocardial infarction recurrence at 30 days, with a significant increase in major bleeds.53 Thus pre-treatment with GPI inhibitors is not recommended.1
Proposed ‘decision-making’ scheme for pre-treatment with a P2Y12 inhibitor
We propose a decision-making scheme for pre-treatment in NSTE ACS patients based on the ESC stratification of the ischaemic risk,1 on the timing of the coronary angiography and on the haemorrhagic risk, assessed by the CRUSADE score,54 choosing a cut-off value of 50 that identifies patients at high risk of major bleeds.
Time to invasive strategy is longer than recommended in a significant amount of patients in Italy,55 in Europe56,57 and in the USA.58 Sometime this deferral could be related to associated clinical conditions that recommend stabilization or a more thorough diagnosis before performing coronary angiography; in the majority of cases, however, the delay stems from the need to transfer the patient in hospitals with cath labs.
Patients at very high ischaemic risk
In case of invasive intervention within 2 h, the oral load of P2Y12 inhibitor will be ineffective at the time of the procedure, and it would therefore appear to be preferable to use GPI if needed, given also their faster resolution of the effect in case of need of a surgical treatment. However, pre-treatment with ticagrelor or prasugrel is not excluded, mainly when the ischaemic risk is far greater than the haemorrhagic risk and the likelihood of surgery is not high.
Patients at high or moderate ischaemic risk
In case of very high haemorrhagic risk, identified by a CRUSADE score ≥ 50, pre-treatment is usually not recommended (red box), and only if the time to the coronary angiography is longer can pre-treatment be considered in selected cases (orange box) (Figure 1).
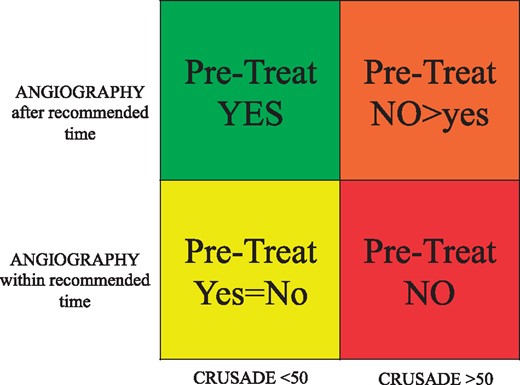
Figure 1
Pre-treatment with P2Y12 inhibitors in non ST-segment elevation acute coronary syndromes at moderate/high risk.
In case of a CRUSADE score <50 pre-treatment is not mandatory but however allowed (yellow box) if coronary angiography will be performed within the recommended time; if the angiography is delayed, pre-treatment with P2Y12 inhibitors would appear to be appropriate (green box).
Patients at low ischaemic risk
In patients with NSTE ACS at low ischaemic risk pre-treatment with P2Y12 inhibitors is not recommended.1
Anticoagulants
The anticoagulant of choice in NSTE ACS should be fondaparinux, due to its more favourable efficacy and safety profile compared with UFH and enoxaparin.1,59,60 In patients pre-treated with fondaparinux an additional bolus of standard-dose UFH must be administered at the time of PCI.
Enoxaparin and UFH are recommended when fondaparinux is not available.13 There are no conclusive data regarding the superiority of one drug over the other.61 In a meta-analysis of over 30 000 patients, enoxaparin compared with UFH determined a slight decrease in the composite endpoint of death and myocardial infarction at 30 days without differences in terms of major bleeds.62 In patients pre-treated with enoxaparin is strongly recommended to avoid to switch to UFH, unfortunately frequently done,55 due to a higher risk of ischaemic and haemorrhagic complications.63 UFH is particularly indicated in patients with severe renal insufficiency.
In the ACUITY study64 bivalirudin was non-inferior to UFH in the reduction of ischaemic events, reducing also major bleeds, but it has to be administered only at the time of the PCI. The usefulness of continuing its infusion after PCI in order to reduce the risk of intra-stent thrombosis was recently questioned.22
Anticoagulation should be discontinued after PCI, except in those patients in whom it has a specific indication.
In patients with NSTE ACS candidates to coronary angiography while on chronic OAT with vitamin K inhibitors or NOA there are still no consistent data. OAT can be stopped and replaced by UFH or enoxaparin, or could be continued at reduced dosages, in order to reduce the risk of both thromboembolic and haemorrhagic events. It is not necessary to administer UFH during PCI if the INR value is greater than 2.5, whereas in case of NOA treatment, administration of an additional intravenous bolus of UFH is recommended.1,23,24
Anti-ischaemic drugs
Beta-blockers
The administration of beta-blockers in NSTE ACS patients demonstrated to reduce in-hospital mortality, except that in patients at risk of cardiogenic shock or with unknown left ventricular function.65
Calcium channel-blockers
Diltiazem and verapamil are possible alternatives in case of contraindications to the use of beta-blockers. They can be used to control angina or in case of vasospasm.1
Nitrates
Nitrates are highly effective in reducing angina and are particularly suitable in patients with incomplete blood pressure control. Their usefulness remains limited to symptom control.1
Statins
The evidences in favour of pre-treatment with high doses of statins in case of PCI in patients with NSTE ACS were summarized in a meta-analysis66 that shows how the administration of atorvastatin 80 mg or rosuvastatin 40 mg before PCI is associated with a reduction in the incidence and amount of post-procedural necrosis, as expressed by lower myocardial damage markers levels, and of short-term MACE.
Reloading is also advisable in patients who are already treated with statins.67
Suggested treatment options for NSTE ACS patients are summarized in Tables 2and3.
Table 2Non ST-segment elevation acute coronary syndromes pre-treatment: very high risk
Table 2Non ST-segment elevation acute coronary syndromes pre-treatment: very high risk
Table 3Non ST-segment elevation acute coronary syndromes pre-treatment: moderate/high risk
Table 3Non ST-segment elevation acute coronary syndromes pre-treatment: moderate/high risk
Patients with stable ischaemic heart disease
Antiplatelet drugs
Aspirin pre-treatment is recommended in all PCI candidates, also if there are no specific data available.68
In the lack of studies, ESC guidelines suggest a loading dose of clopidogrel before PCI when coronary anatomy is known, recommending its administration at least 2 h before the procedure;68 guidelines take also into consideration a loading dose of clopidogrel in patients with a high likelihood of coronary stenosis to revascularize.38,68,69 In patients who are already on treatment with clopidogrel, reloading with 600 mg can be considered once angioplasty is planned.
There are no data available on the use of ticagrelor and prasugrel in non-ACS patients, so their administration is not recommended.
Use of GPI should be reserved as rescue therapy in case of intra-procedural thrombotic complications.70
Anticoagulants
In patients with stable ischaemic heart disease the aim of anticoagulant therapy is to reduce the risk of peri-procedural thrombotic complications, and it should therefore only be administered at the time of PCI.
UFH remains the standard of care.71 Enoxaparin can be used as alternative to UFH.72 Bivalirudin should be reserved for patients at very high bleeding risk.73
In stable patients on OAT it is reasonable to continue administration of vitamin K inhibitors, adding a reduced dose of UFH only in case of radial approach. The great handling of NOAs makes it easy to temporarily stop treatment.23,24,74
Anti-ischaemic drugs
In general, there is no specific need of anti-ischaemic treatment before a revascularization procedure, if not those suited to the patient's specific clinical condition.
Statins
Statins are recommended with the aim of keeping C-LDL levels below 70 mg/dL.68 Pre-procedural administration in stable patients is thought to be effective to prevent contrast-induced kidney disease.75
A recent meta-analysis76 showed that pre-treatment with high doses of high-efficacy statin is associated with a reduction in the risk of peri-procedural myocardial necrosis, and a reduction in short-term MACE.
It would therefore appear advisable to administer an oral loading dose of 80 mg of atorvastatin or 20–40 mg of rosuvastatin before elective percutaneous revascularization procedure. Reloading is appropriate in patients already on therapy with another statin.77
Suggested treatment options for stable ischaemic heart disease patients are summarized in Table 4.
Table 4Stable ischaemic heart disease pre-treatment
Table 4Stable ischaemic heart disease pre-treatment
Patients candidates to coronary artery bypass grafting
Most patients who are candidates to CABG are on treatment with antiplatelet, anticoagulant, beta-blocker and statin therapy, whose pre-operative administration must be managed in order to maintain their cardio-protective effects, but avoiding to increase bleeding or hypotension.
Antiplatelet drugs
Antiplatelet drugs improve short- and long-term outcomes even in patients undergoing CABG;78,79 bleeding is however a serious and common complication80,81 that implies an additional risk of further adverse events.82–84
Pre-operative discontinuation of aspirin is considered to be risky in patients with ACS or with coronary stents,85 and it should only be considered in case of a very high risk of bleeding or in patients who refuse transfusions, stopping treatment three days before the procedure.86,87
In patients with stable coronary disease, the benefits of continuing therapy with aspirin up to the day of the procedure are less well defined. It was highlighted a slight increase in the risk of bleeding without improving the early graft patency rate.88 The ATACAS trial89 did not reveal any differences in major bleeds with the pre-operative use of aspirin, nor a reduction in thrombotic events or in mortality, possibly due to the low risk of the population studied.
Prasugrel compared with clopidogrel significantly increases post-operative bleedings, including fatal ones; however, after discontinuation of the drug, post-operative mortality was lower than for patients treated with clopidogrel.90
Ticagrelor demonstrated peri-operative bleeding risk similar to clopidogrel,91 but mortality in patients treated 3–5 days after the last administered dose was significantly lower.92 Ticagrelor has a reversible binding with platelets, and may remain in circulation for a long time, inhibiting also transfused platelets.93 A specific antidote is currently being developed.94
It may be appropriate to monitor platelet inhibition with dedicated tests, in order to limit the antiplatelet discontinuation period to 1–2 days.95,96
These are the ESC guidelines suggestions:37,68in case of high or very high risk of haemorrhage:
aspirin should be maintained for the entire surgical period;
clopidogrel and ticagrelor should be discontinued 5 days before the procedure;
prasugrel should be discontinued 7 days before;
in case of high or very high thrombotic risk (clinical and/or anatomical):
aspirin should be maintained for the entire surgical period;
in emergency, discontinuing the P2Y12 inhibitor is not recommended and all possible measures must be taken to reduce the risk of bleeding;
in case of urgent surgery, consider to perform the procedure after 1-2 days of discontinuation.
In case of very high both thrombotic and ischaemic risk, ‘bridging’ strategies with short half-life intravenous anti-platelet drugs were evaluated:
discontinuation of clopidogrel 5 days before the procedure and administration of tirofiban or eptifibatide i.v. up to 4 h before;97
discontinuation of thienopyridine (99% clopidogrel) 48 h before the procedure and administration of intravenous cangrelor up to 1–6 h before.98
Replacing double antiplatelet therapy with heparin is not recommended.
A P2Y12 inhibitor should be administered as soon as possible after the procedure, as it improves graft patency and outcome at 30 days.99,100
Anticoagulants
In patients treated with vitamin K inhibitors, normal INR values must be restored before an elective procedure. The use of low molecular weight heparin as a therapeutic bridge may increase the risk of peri-procedural bleeding.100 In case of emergency/urgency, vitamin K and/or transfusions of fresh plasma or prothrombin complex concentrates may be administered.101
If a NOA is used, it should be discontinued 48–96 h before a scheduled procedure, taking into account the patient's kidney function and the drug used,102 without bridging with heparin.74,100,103
Laboratory tests to measure NOA effects have not yet been validated, as the relationship between the value of the measured parameter and the risk of bleeding is not known.102
In case of urgent heart surgery, it would seem preferable to wait until the NOAs are no longer effective. In case of emergency procedures, activated prothrombin complexes may be used.104
Specific inhibitors have so far been studied on a very limited number of patients. Idarucizumab is an antibody fragment that in a few minutes overrides the effect of dabigatran,105 whereas Andexanet inhibits the effect of anti-Xa NOA.106
The administration of NOAs should not be restarted earlier than 48–72 h after the procedure, and there are no data available on use at reduced dosages.
Beta-blockers
The enthusiasm on the use of these drugs was curbed by the results of a meta-analysis,107 by the results of a Texas Heart Surgery Society database,108 and by a retrospective analysis of the data of over 500 000 patients without recent myocardial infarction109: pre-operative use did not lead to a mortality reduction, while slightly increased the incidence of atrial fibrillation; the underlying mechanism is possibly related to hypotension.
Statins
Statins reduce the development of venous graft disease110; pleiotropic effects are associated with a reduction in adverse clinical events and to cardiovascular protection.111,112
Despite these premises, a review113 on pre-operative treatment indicated as the only result a reduction in the incidence of post-operative atrial fibrillation and consequently of the duration of hospitalization. There were no significant effects on mortality, stroke, peri-operative infarction or kidney disease.
Conclusions
The antithrombotic drugs administration before coronary angiography in patients with coronary disease on the one hand may make it possible to bring forward optimal therapy but on the other it may expose to risk of bleeding that, particularly in patients with ACS, can weigh heavily on prognosis, even more so than the theoretical benefit of pre-treatment.
In NSTE ACS patients in particular, we suggest a ‘selective pre-treatment’ with P2Y12 inhibitors, guided by a careful assessment of both ischaemic and haemorrhagic risk, whilst also taking into consideration the actual time delay before the coronary angiography.
Many of the issues regarding this topic could be solved by early access to coronary angiography, particularly in patients at greatest risk of events.
Consensus Document Approval Faculty
Abrignani Maurizio Giuseppe, Alunni Gianfranco, Amodeo Vincenzo, Angeli Fabio, Aspromonte Nadia, Audo Andrea, Azzarito Michele, Battistoni Ilaria, Bianca Innocenzo, Bisceglia Irma, Bongarzoni Amedeo, Bonvicini Marco, Cacciavillani Luisa, Calculli Giancarlo Giacinto, Caldarola Pasquale, Capecchi Alessandro, Caretta Giorgio, Carmina Maria Gabriella, Casazza Franco, Casu Gavino, Cemin Roberto, Chiarandà Giacomo, Chiarella Francesco, Chiatto Mario, Cibinel Gian Alfonso, Ciccone Marco Matteo, Cicini Maria Paola, Clerico Aldo, D'Agostino Carlo, De Luca Giovanni, De Maria Renata, Del Sindaco Donatella, Di Fusco Stefania Angela, Di Lenarda Andrea, Di Tano Giuseppe, Egidy Assenza Gabriele, Egman Sabrina, Enea Iolanda, Fattirolli Francesco, Favilli Silvia, Ferraiuolo Giuseppe, Francese Giuseppina Maura, Gabrielli Domenico, Giardina Achille, Greco Cesare, Gregorio Giovanni, Iacoviello Massimo, Khoury Georgette, Lucà Fabiana, Lukic Vjerica, Macera Francesca, Marini Marco, Masson Serge, Maurea Nicola, Mazzanti Marco, Mennuni Mauro, Menotti Alberto, Mininni Nicola, Moreo Antonella, Mortara Andrea, Mureddu Gian Francesco, Murrone Adriano, Nardi Federico, Navazio Alessandro, Nicolosi Gian Luigi, Oliva Fabrizio, Parato Vito Maurizio, Parrini Iris, Patanè Leonardo, Pini Daniela, Pino Paolo Giuseppe, Pirelli Salvatore, Procaccini Vincenza, Pugliese Francesco Rocco, Pulignano Giovanni, Radini Donatella, Rao Carmelo Massimiliano, Riccio Carmine, Roncon Loris, Rossini Roberta, Ruggieri Maria Pia, Rugolotto Matteo, Sanna Fabiola, Sauro Rosario, Severi Silva, Sicuro Marco, Silvestri Paolo, Sisto Francesco, Tarantini Luigi, Uguccioni Massimo, Urbinati Stefano, Valente Serafina, Vatrano Marco, Vianello Gabriele, Vinci Eugenio, Zuin Guerrino.
Conflict of Interest: Dr. Roberto Caporale reports honoraria for consulting from Lilly and Boehringer Ingelheim. Dr. Alberto Menozzi reports honoraria for lectures and consulting from Astra-Zeneca, Abbott Vascular, Bayer, Correvio, Daiichi-Sankyo, Medtronic, MSD, The Medicines Company. Giuseppe Musumeci reports honoraria for lectures from Daiichi Sankyo, Astra Zeneca, Menarini, Servier and Abbott Vascular. Prof. Giuseppe Tarantini reports honoraria for lectures from Boston Scientific, St. Jude Medical, Philips Volcano, Medtronic and Abbott Vascular.
References
1Roffi
M
, Patrono
C
, Collet
JP
, Mueller
C
, Valgimigli
M
, Andreotti
F
, Bax
JJ
, Borger
MA
, Brotons
C
, Chew
DP
, Gencer
B
, Hasenfuss
G
, Kjeldsen
K
, Lancellotti
P
, Landmesser
U
, Mehilli
J
, Mukherjee
D
, Storey
RF
, Windecker
S
.
2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation
.
Eur Heart J
2016
;
37
:
267
–
315
.
2Steg
PG
, James
SK
, Atar
D
, Badano
LP
, Blömstrom-Lundqvist
C
, Borger
MA
, Di Mario
C
, Dickstein
K
, Ducrocq
G
, Fernandez-Aviles
F
, Gershlick
AH
, Giannuzzi
P
, Halvorsen
S
, Huber
K
, Juni
P
, Kastrati
A
, Knuuti
J
, Lenzen
MJ
, Mahaffey
KW
, Valgimigli
M
, van't Hof
A
, Widimsky
P
, Zahger
D
.
ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation
.
Eur Heart J
2012
;
33
:
2569
–
2619
.
3Sabatine
MS
, Cannon
CP
, Gibson
CM
, Lopez-Sendon
JL
, Montalescot
G
, Theroux
P
, Claeys
MJ
, Cools
F
, Hill
KA
, Skene
AM
, McCabe
CH
, Braunwald
E
;
CLARITY-TIMI 28 Investigators
.
Addition of clopidogrel to aspirin and fibrinolytic therapy for myocardial infarction with ST-segment elevation
.
N Engl J Med
2005
;
352
:
1179
–
1189
.
4Sabatine
MS
, Cannon
CP
, Gibson
CM
, Lopez-Sendon
JL
, Montalescot
G
, Theroux
P
, Lewis
BS
, Murphy
SA
, McCabe
CH
, Braunwald
E
.
Effect of clopidogrel pretreatment before percutaneous coronary intervention in patients with ST-elevation myocardial infarction treated with fibrinolytics: the PCI-CLARITY study
.
JAMA
2005
;
294
:
1224
–
1232
.
5Zeymer
U
, Arntz
HR
, Mark
B
, Fichtlscherer
S
, Werner
G
, Scholler
R
, Zahn
R
, Diller
F
, Darius
H
, Dill
T
, Huber
K
.
Efficacy and safety of a high loading dose of clopidogrel administered prehospitally to improve primary percutaneous coronary intervention in acute myocardial infarction: the randomized CIPAMI trial
.
Clin Res Cardiol
2012
;
101
:
305
–
312
.
6Ducci
K
, Grotti
S
, Falsini
G
, Angioli
P
, Liistro
F
, Mando
M
, Porto
I
, Bolognese
L
.
Comparison of pre-hospital 600 mg or 900 mg vs. peri-interventional 300 mg clopidogrel in patients with ST-elevation myocardial infarction undergoing primary coronary angioplasty. The Load&Go randomized trial
.
Int J Cardiol
2013
;
168
:
4814
–
4816
.
7Bellemain-Appaix
A
, O’connor
SA
, Silvain
J
, Cucherat
M
, Beygui
F
, Barthélémy
O
, Collet
J-P
, Jacq
L
, Bernasconi
F
, Montalescot
G
;
for the ACTION Study Group
.
Association of clopidogrel pretreatment with mortality, cardiovascular events, and major bleeding among patients undergoing percutaneous coronary intervention: a systematic review and meta-analysis
.
JAMA
2012
;
308
:
2507
–
2516
.
8Wiviott
SD
, Braunwald
E
, McCabe
CH
, Montalescot
G
, Ruzyllo
W
, Gottlieb
S
, Neumann
F-J
, Ardissino
D
, De Servi
S
, Murphy
SA
, Riesmeyer
J
, Weerakkody
G
, Gibson
CM
, Antman
EM
.
Prasugrel versus clopidogrel in patients with acute coronary syndromes
.
N Engl J Med
2007
;
357
:
2001
–
2015
.
9Wallentin
L
, Becker
RC
, Budaj
A
, Cannon
CP
, Emanuelsson
H
, Held
C
, Horrow
J
, Husted
S
, James
S
, Katus
H
, Mahaffey
KW
, Scirica
BM
, Skene
A
, Steg
PG
, Storey
RF
, Harrington
RA
;
PLATO Investigators
.
Ticagrelor versus clopidogrel in patients with acute coronary syndromes
.
N Engl J Med
2009
;
361
:
1045
–
1057
.
10Montalescot
G
, Wiviott
SD
, Braunwald
E
, Murphy
SA
, Gibson
CM
, McCabe
CH
, Antman
EM
;
TRITON-TIMI 38 Investigators
.
Prasugrel compared with clopidogrel in patients undergoing percutaneous coronary intervention for ST-elevation myocardial infarction (TRITON-TIMI 38): double-blind, randomised controlled trial
.
Lancet
2009
;
373
:
723
–
731
.
11Steg
PG
, James
S
, Harrington
RA
, Ardissino
D
, Becker
RC
, Cannon
CP
, Emanuelsson
H
, Finkelstein
A
, Husted
S
, Katus
H
, Kilhamn
J
, Olofsson
S
, Storey
RF
, Weaver
WD
, Wallentin
L
;
PLATO Study Group
.
Ticagrelor versus clopidogrel in patients with ST-elevation acute coronary syndromes intended for reperfusion with primary percutaneous coronary intervention: a Platelet Inhibition and Patient Outcomes (PLATO) trial subgroup analysis
.
Circulation
2010
Nov 23;
122
:
2131
–
2141
.
12Montalescot
G
, Van’t Hof
AW
, Lapostolle
F
, Silvain
J
, Lassen
JF
, Bolognese
L
, Cantor
WJ
, Cequier
A
, Chettibi
M
, Goodman
SG
, Hammett
CJ
, Huber
K
, Janzon
M
, Merkely
B
, Storey
RF
, Zeymer
U
, Stibbe
O
, Ecollan
P
, Heutz
WM
, Swahn
E
, Collet
JP
, Willems
FF
, Baradat
C
, Licour
M
, Tsatsaris
A
, Vicaut
E
, Hamm
CW
;
ATLANTIC Investigators
.
Prehospital ticagrelor in ST-segment elevation myocardial infarction
.
N Engl J Med
2014
;
371
:
1016
–
1027
.
13De Luca
G
, Navarese
E
, Marino
P.
Risk profile and benefits from Gp IIb-IIIa inhi- bitors among patients with ST-segment elevation myocardial infarction treated with primary angioplasty: a meta-regression analysis of randomized trials
.
Eur Heart J
2009
;
30
:
2705
–
2713
.
14Mehran
R
, Lansky
AJ
, Witzenbichler
B
, Guagliumi
G
, Peruga
JZ
, Brodie
BR
, Dudek
D
, Kornowski
R
, Hartmann
F
, Gersh
BJ
, Pocock
SJ
, Wong
SC
, Nikolsky
E
, Gambone
L
, Vandertie
L
, Parise
H
, Dangas
GD
, Stone
GW
;
HORIZONS-AMI Trial Investigators
.
Bivalirudin in patients undergoing primary angioplasty for acute myocardial infarction (HORIZONS-AMI): 1-year results of a randomised controlled trial
.
Lancet
2009
;
374
:
1149
–
1159
.
15Mehilli
J
, Kastrati
A
, Schulz
S
, Früngel
S
, Nekolla
SG
, Moshage
W
, Dotzer
F
, Huber
K
, Pache
J
, Dirschinger
J
, Seyfarth
M
, Martinoff
S
, Schwaiger
M
, Schömig
A
;
Bavarian Reperfusion Alternatives Evaluation-3 (BRAVE-3) Study Investigators
.
Abciximab in patients with acute ST-segment-elevation myocardial infarction undergoing primary percutaneous coronary intervention after clopidogrel loading: a randomized double-blind trial
.
Circulation
2009
;
119
:
1933
–
1940
.
16Ellis
SG
, Tendera
M
, de Belder
MA
, van Boven
AJ
, Widimsky
P
, Janssens
L
, Andersen
HR
, Betriu
A
, Savonitto
S
, Adamus
J
, Peruga
JZ
, Kosmider
M
, Katz
O
, Neunteufl
T
, Jorgova
J
, Dorobantu
M
, Grinfeld
L
, Armstrong
P
, Brodie
BR
, Herrmann
HC
, Montalescot
G
, Neumann
FJ
, Effron
MB
, Barnathan
ES
, Topol
EJ
;
FINESSE Investigators
.
Facilitated PCI in patients with ST-elevation myocardial infarction
.
N Eng J Med
2008
;
358
:
2205
–
2217
.
17Herrmann
HC
, Lu
J
, Brodie
BR
, Armstrong
PW
, Montalescot
G
, Betriu
A
, Neuman
FJ
, Effron
MB
, Barnathan
ES
, Topol
EJ
, Ellis
SG
;
FINESSE Investigators
.
Benefit of facilitated percutaneous coronary intervention in high-risk ST-segment elevation myocardial infarction patients presenting to nonpercutaneous coronary intervention hospitals
.
JACC Cardiovasc Interv
2009
;
2
:
917
–
924
.
18Montalescot
G
, Zeymer
U
, Silvain
J
, Boulanger
B
, Cohen
M
, Goldstein
P
, Ecollan
P
, Combes
X
, Huber
K
, Pollack
C
Jr, Bénezet
JF
, Stibbe
O
, Filippi
E
, Teiger
E
, Cayla
G
, Elhadad
S
, Adnet
F
, Chouihed
T
, Gallula
S
, Greffet
A
, Aout
M
, Collet
JP
, Vicaut
E
;
ATOLL Investigators
.
Intravenous enoxaparin or unfractionated heparin in primary percutaneous coronary intervention for ST-elevation myocardial infarction: the international randomised open-label ATOLL trial
.
Lancet
2011
;
378
:
693
–
703
.
19Stone
GW
, Witzenbichler
B
, Guagliumi
G
, Peruga
JZ
, Brodie
BR
, Dudek
D
, Kornowski
R
, Hartmann
F
, Gersh
BJ
, Pocock
SJ
, Dangas
G
, Wong
SC
, Kirtane
AJ
, Parise
H
, Mehran
R
;
HORIZONS-AMI Trial Investigators
.
Bivalirudin during primary PCI in acute myocardial infarction
.
N Engl J Med
2008
;
358
:
2218
–
2230
.
20Steg
PG
, van 'T Hof
A
, Hamm
CW
, Peruga
JZ
, Brodie
BR
, Dudek
D
, Kornowski
R
, Hartmann
F
, Gersh
BJ
, Pocock
SJ
, Dangas
G
, Wong
SC
, Kirtane
AJ
, Parise
H
, Mehran
R
;
HORIZONS-AMI Trial Investigators
.
Bivalirudin started during emergency transport for primary PCI
.
N Engl J Med
2013
;
369
:
2207
–
2217
.
21Shahzad
A
, Kemp
I
, Mars
C
, Wilson
K
, Roome
C
, Cooper
R
, Andron
M
, Appleby
C
, Fisher
M
, Khand
A
, Kunadian
B
, Mills
JD
, Morris
JL
, Morrison
WL
, Munir
S
, Palmer
ND
, Perry
RA
, Ramsdale
DR
, Velavan
P
, Stables
RH
;
HEAT-PPCI trial investigators
.
Unfractionated heparin versus bivalirudin in primary percutaneous coronary intervention (HEAT-PPCI): an open-label, single centre, randomised controlled trial
.
Lancet
2014
;
384
:
1849
–
1858
.
22Valgimigli
M
, Frigoli
E
, Leonardi
S
, Rothenbühler
M
, Gagnor
A
, Calabrò
P
, Garducci
S
, Rubartelli
P
, Briguori
C
, Andò
G
, Repetto
A
, Limbruno
U
, Garbo
R
, Sganzerla
P
, Russo
F
, Lupi
A
, Cortese
B
, Ausiello
A
, Ierna
S
, Esposito
G
, Presbitero
P
, Santarelli
A
, Sardella
G
, Varbella
F
, Tresoldi
S
, de Cesare
N
, Rigattieri
S
, Zingarelli
A
, Tosi
P
, van 't Hof
A
, Boccuzzi
G
, Omerovic
E
, Sabaté
M
, Heg
D
, Jüni
P
, Vranckx
P
;
MATRIX Investigators
.
Bivalirudin or Unfractionated Heparin in Acute Coronary Syndromes
.
N Engl J Med
2015
;
373
:
997
–
1009
.
23Rubboli
A
, Faxon
DP
, Juhani Airaksinen
KE
, Schlitt
A
, Marín
F
, Bhatt
DL
, Lip
GY.
The optimal management of patients on oral anticoagulation undergoing coronary artery stenting. The 10th Anniversary Overview
.
Thromb Haemost
2014
;
112
:
1080
–
1087
.
24Lip
GY
, Windecker
S
, Huber
, Kirchhof
P
, Marin
F
, ten Berg
JM
, Haeusler
KG
, Boriani
G
, Capodanno
D
, Gilard
M
, Zeymer
U
, Lane
D
, Storey
RF
, Bueno
H
, Collet
JP
, Fauchier
L
, Halvorsen
S
, Lettino
M
, Morais
J
, Mueller
C
, Potpara
TS
, Rasmussen
LH
, Rubboli
A
, Tamargo
J
, Valgimigli
M
, Zamorano
JL
.
Management of antithrombotic therapy in atrial fibrillation patients presenting with acute coronary syndrome and/or undergoing percutaneous coronary or valve interventions: a joint consensus document of the European Society of Cardiology working group on thrombosis, European Heart Rhythm Association (EHRA), European Association of Percutaneous Cardiovascular Interventions (EAPCI) and European Association of Acute Cardiac Care (ACCA) endorsed by the Heart Rhythm Society (HRS) and Asia-Pacific Heart Rhythm Society (APHRS)
.
Eur Heart J
2014
;
35
:
3155
–
3179
.
25Yusuf
S
, Peto
R
, Lewis
J
, Collins
R
, Sleight
P
.
Beta-blockade during and after myocardial infarction: an overview of the randomized trials
.
Prog Cardiovasc Dis
1985
;
27
:
335
–
371
.
26
Randomised trial of intravenous atenolol among 16 027 cases of suspected acute myocardial infarction: ISIS-1. First International Study of Infarct Survival Collaborative Group
.
Lancet
1986
;
2
:
57
–
66
.
27Chen
ZM
, Pan
HC
, Chen
YP
, Peto
R
, Collins
R
, Jiang
LX
, Xie
JX
, Liu
LS
;
COMMIT (ClOpidogrel and Metoprolol in Myocardial Infarction Trial) collaborative group
.
Early intravenous then oral metoprolol in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial
.
Lancet
2005
;
366
:
1622
–
1632
.
28Kontos
MC
, Diercks
DB
, Ho
PM
, Wang
TY
, Chen
AY
, Roe
MT.
Treatment and outcomes in patients with myocardial infarction treated with acute beta-blocker therapy: results from the American College of Cardiology’s NCDRw
.
Am Heart J
2011
;
161
:
864
–
870
.
29Yusuf
S
, Held
P
, Furberg
C.
Update of effects of calcium antagonists in myocardial infarction or angina in light of the second Danish Verapamil Infarction Trial (DAVIT-II) and other recent studies
.
Am J Cardiol
1991
;
67
:
1295
–
1297
.
30Ray
KK
, Cannon
CP.
The potential relevance of the multiple lipid-independent (pleiotropic) effects of statins in the management of acute coronary syndromes
.
J Am Coll Cardiol
2005
;
46
:
1425
–
1433
.
31Kim
JS
, Kim
J
, Choi
D
, Lee
CJ
, Lee
SH
, Ko
YG
, Hong
MK
, Kim
BK
, Oh
SJ
, Jeon
DW
, Yang
JY
, Cho
JR
, Lee
NH
, Cho
YH
, Cho
DK
, Jang
Y
.
Efficacy of high-dose atorvastatin loading before primary percutaneous coronary intervention in ST-segment elevation myocardial infarction: the STATIN STEMI trial
.
JACC Cardiovasc Interv
2010
;
3
:
332
–
339
.
32Liu
HL
, Yang
Y
, Yang
SL
, et al.
Administration of a loading dose of atorvastatin before percutaneous coronary intervention prevents inflammation and reduces myocardial injury in STEMI patients: a randomized clinical study
.
Clin Ther
2013
;
35
:
261
–
272
.
33Lyu
T
, Zhao
Y
, Zhang
T
, Luo
JP
, Li
H
, Jing
LM
, Shen
ZQ
.
Effect of statin pretreatment on myocardial perfusion in patients undergoing primary percutaneous coronary intervention: a systematic review and meta-analysis
.
Clin Cardiol
2013
;
36
:
E17
–
E24
.
34Kim
JW
, Yun
KH
, Kim
EK
, Joe
DY
, Ko
JS
, Rhee
SJ
, Lee
EM
, Yoo
NJ
, Kim
NH
, Oh
SK
, Jeong
JW
.
Effect of high dose rosuvastatin loading before primary percutaneous coronary intervention on infarct size in patients with ST-segment elevation myocardial infarction
.
Korean Circ J
2014
;
44
:
76
–
81
.
35Zhou
SS
, Tian
F
, Chen
YD
, Wang
J
, Sun
ZJ
, Guo
J
, Jin
QH
.
Combination therapy reduces the incidence of no-reflow after primary per-cutaneous coronary intervention in patients with ST-segment elevation acute myocardial infarction
.
J Geriatr Cardiol
2015
;
12
:
135
–
142
.
36Agenzia Italiana del Farmaco
. Modifica alla Nota 13 di cui alla Determina del 26 marzo 2013. Gazzetta Ufficiale – serie generale - n. 156 del 08/07/2014.
37Hamm
CW
, Bassand
JP
, Agewall
S
, Bax
J
, Boersma
E
, Bueno
H
, Caso
P
, Dudek
D
, Gielen
S
, Huber
K
, Ohman
M
, Petrie
MC
, Sonntag
F
, Uva
MS
, Storey
RF
, Wijns
W
, Zahger
D
;
ESC Committee for Practice Guidelines
.
ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: the task force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC)
.
Eur Heart J
2011
;
32
:
2999
–
3054
.
38Patrono
C
, Andreotti
F
, Arnesen
H
, Badimon
L
, Baigent
C
, Collet
JP
, De Caterina
R
, Gulba
D
, Huber
K
, Husted
S
, Kristensen
SD
, Morais
J
, Neumann
FJ
, Rasmussen
LH
, Siegbahn
A
, Steg
PG
, Storey
RF
, Van deWerf
F
, Verheugt
F
.
Antiplatelet agents for the treatment and prevention of atherothrombosis
.
Eur Heart J
2011
;
32
:
2922
–
2932
.
39The RISC Group
.
Risk of myocardial infarction and death during treatment with low dose aspirin and intravenous heparin in men with unstable coronary artery disease
.
Lancet
1990
;
336
:
827
–
830
.
40Lewis
HD
Jr, Davis
JW
, Archibald
DG
, Steinke
WE
, Smitherman
TC
, Doherty
JE
3rd, Schnaper
HW
, LeWinter
MM
, Linares
E
, Pouget
JM
, Sabharwal
SC
, Chesler
E
, DeMots
H
.
Protective effects of aspirin against acute myocardial infarction and death in men with unstable angina. Results of a Veterans Administration cooperative study
.
N Engl J Med
1983
;
309
:
396
–
403
.
41Theroux
P
, Ouimet
H
, McCans
J
, Latour
JG
, Joly
P
, Levy
G
, Pelletier
E
, Juneau
M
, Stasiak
J
, deGuise
P
, Pelletier
GB
, Rinzler
D
, Waters
DD
.
Aspirin, heparin, or both to treat acute unstable angina
.
N Engl J Med
1988
;
319
:
1105
–
1111
.
42Cairns
JA
, Gent
M
, Singer
J
, Finnie
KJ
, Froggatt
GM
, Holder
DA
, Jablonsky
G
, Kostuk
WJ
, Melendez
LJ
, Myers
MG
, Sackett
DL
, Sealey
BJ
, Tanser
PH
.
Aspirin, sulfinpyrazone, or both in unstable angina. Results of a Canadian multicenter trial
.
N Engl J Med
1985
;
313
:
1369
–
1375
.
43Antithrombotic Trialists’ Collaboration
.
Collaborative meta-analysis of randomized trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients
.
BMJ
2002
;
324
:
71
–
86
.
44Mehta
SR
, Yusuf
S
, Peters
RJ
, Bertrand
ME
, Lewis
BS
, Natarajan
MK
, Malmberg
K
, Rupprecht
H
, Zhao
F
, Chrolavicius
S
, Copland
I
, Fox
KA
.
Effects of pretreatment with clopidogrel and aspirin followed by long-term therapy in patients undergoing percutaneous coronary intervention: the PCI-CURE study
.
Lancet
2001
;
358
:
527
–
533
.
45Montalescot
G
, Bolognese
L
, Dudek
D
, Goldstein
P
, Hamm
C
, Tanguay
JF
, ten Berg
JM
, Miller
DL
, Costigan
TM
, Goedicke
J
, Silvain
J
, Angioli
P
, Legutko
J
, Niethammer
M
, Motovska
Z
, Jakubowski
JA
, Cayla
G
, Visconti
LO
, Vicaut
E
, Widimsky
P
;
ACCOAST Investigators
.
Pretreatment with prasugrel in non-ST-segment elevation acute coronary syndromes
.
N Engl J Med
2013
;
369
:
999
–
1010
.
46Lindholm
D
, Varenhorst
C
, Cannon
CP
, Harrington
RA
, Himmelmann
A
, Maya
J
, Husted
S
, Steg
PG
, Cornel
JH
, Storey
RF
, Stevens
SR
, Wallentin
L
, James
SK
.
Ticagrelor vs. clopidogrel in patients with non-ST-elevation acute coronary syndrome with or without revascularization: results from the PLATO trial
.
Eur Heart J
2014
;
35
:
2083
–
2093
.
47Bhatt
DL
, Lincoff
AM
, Gibson
CM
, Stone
GW
, McNulty
S
, Montalescot
G
, Kleiman
NS
, Goodman
SG
, White
HD
, Mahaffey
KW
, Pollack
CV
Jr, Manoukian
SV
, Widimsky
P
, Chew
DP
, Cura
F
, Manukov
I
, Tousek
F
, Jafar
MZ
, Arneja
J
, Skerjanec
S
, Harrington
RA
;
CHAMPION PLATFORM Investigators
.
Intravenous platelet blockade with cangrelor during PCI
.
N Engl J Med
2009
;
361
:
2330
–
2341
.
48Harrington
RA
, Stone
GW
, McNulty
S
, White
HD
, Lincoff
AM
, Gibson
CM
, Pollack
CV
Jr, Montalescot
G
, Mahaffey
KW
, Kleiman
NS
, Goodman
SG
, Amine
M
, Angiolillo
DJ
, Becker
RC
, Chew
DP
, French
WJ
, Leisch
F
, Parikh
KH
, Skerjanec
S
, Bhatt
DL
.
Platelet inhibition with cangrelor in patients undergoing PCI
.
N Engl J Med
2009
;
361
:
2318
–
2329
.
49Bhatt
DL
, Stone
GW
, Mahaffey
KW
, Gibson
CM
, Steg
PG
, Hamm
CW
, Price
MJ
, Leonardi
S
, Gallup
D
, Bramucci
E
, Radke
PW
, Widimský
P
, Tousek
F
, Tauth
J
, Spriggs
D
, McLaurin
BT
, Angiolillo
DJ
, Généreux
P
, Liu
T
, Prats
J
, Todd
M
, Skerjanec
S
, White
HD
, Harrington
RA
;
CHAMPION PHOENIX Investigators
.
Effect of platelet inhibition with cangrelor during PCI on ischemic events
.
N Engl J Med
2013
;
368
:
1303
–
1313
.
50Steg
PG
, Bhatt
DL
, Hamm
CW
, Stone
GW
, Gibson
CM
, Mahaffey
KW
, Leonardi
S
, Liu
T
, Skerjanec
S
, Day
JR
, Iwaoka
RS
, Stuckey
TD
, Gogia
HS
, Gruberg
L
, French
WJ
, White
HD
, Harrington
RA
;
CHAMPION Investigators
.
Effect of cangrelor on peri-procedural out- comes in percutaneous coronary interventions: a pooled analysis of patient-level data
.
Lancet
2013
;
382
:
1981
–
1992
.
51Stone
GW
, Bertrand
ME
, Moses
JW
, Ohman
EM
, Lincoff
AM
, Ware
JH
, Pocock
SJ
, McLaurin
BT
, Cox
DA
, Jafar
MZ
, Chandna
H
, Hartmann
F
, Leisch
F
, Strasser
RH
, Desaga
M
, Stuckey
TD
, Zelman
RB
, Lieber
IH
, Cohen
DJ
, Mehran
R
, White
HD
.
Routine upstream initiation vs deferred selective use of glycoprotein IIb/IIIa inhibitors in acute coronary syndromes: the ACUITY timing trial
.
JAMA
2007
;
297
:
591
–
602
.
52Giugliano
RP
, White
JA
, Bode
C
, Armstrong
PW
, Montalescot
G
, Lewis
BS
, van’t Hof
A
, Berdan
LG
, Lee
KL
, Strony
JT
, Hildemann
S
, Veltri
E
, Van de Werf
F
, Braunwald
E
, Harrington
RA
, Califf
RM
, Newby
LK
.
Early versus delayed, provisional eptifibatide in acute coronary syndromes
.
N Engl J Med
2009
;
360
:
2176
–
2190
.
53De Luca
G
, Navarese
EP
, Cassetti
E
, Verdoia
M
, Suryapranata
H.
Meta-analysis of randomized trials of glycoprotein IIb/IIIa inhibitors in high-risk acute coronary syndromes patients undergoing invasive strategy
.
Am J Cardiol
2011
;
107
:
198
–
203
.
54Subherwal
S
, Bach
RG
, Chen
AY
, Gage
BF
, RAO
SV
, Newby
LK
, Wang
TY
, Gibler
WB
, Ohman
EM
, Roe
MT
.
Baseline Risk of Major Bleeding in Non-ST-Segment-Elevation Myocardial Infarction. The CRUSADE (Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA guidelines) Bleeding Score
.
Circulation
2009
;
119
:
1873
–
1882
.
55De Luca
L
, Leonardi
S
, Cavallini
C
, Lucci
D
, Musumeci
G
, Caporale
R
, Abrignani
MG
, Lupi
A
, Rakar
S
, Gulizia
MM
, Bovenzi
FM
, De Servi
S
;
EYESHOT Investigators
.
Contemporary antithrombotic strategies in patients with acute coronary syndromes admitted to cardiac care units in Italy: the EYESHOT study
.
Eur Heart J Acute Cardiovasc Care
2015
;
4
:
441
–
452
.
56Bakhai
A
, Iñiguez
A
, Ferrieres
J
, Schmitt
C
, Sartral
M
, Belger
M
, Zeymer
U
;
APTOR Trial Investigators
.
Treatment patterns in acute coronary syndrome patients in the United Kingdom undergoing PCI
.
EuroIntervention
2011
;
6
:
992
–
996
.
57Puymirat
E
, Taldir
G
, Aissaoui
N
, Lemesle
G
, Lorgis
L
, Cuisset
T
, Bourlard
P
, Maillier
B
, Ducrocq
G
, Ferrieres
J
, Simon
T
, Danchin
N
.
Use of invasive strategy in non-ST-segment elevation myocardial infarction is a major determinant of improved long-term survival: FAST-MI (French Registry of Acute Coronary Syndrome)
.
JACC Cardiovasc Interv
2012
;
5
:
893
–
902
.
58Swanson
N
, Montalescot
G
, Eagle
KA
, Goodman
SG
, Huang
W
, Brieger
D
, Devlin
G
;
GRACE Investigators
.
Delay to angiography and outcomes following presentation with high-risk, non-ST-elevation acute coronary syndromes: results from the Global Registry of Acute Coronary Events
.
Heart
2009
;
95
:
211
–
215
.
59Yusuf
S
, Mehta
SR
, Chrolavicius
S
, Afzal
R
, Pogue
J
, Granger
CB
, Budaj
A
, Peters
RJ
, Bassand
JP
, Wallentin
L
, Joyner
C
, Fox
KA
.
Comparison of fondaparinux and enoxaparin in acute coronary syndromes
.
N Engl J Med
2006
;
354
:
1464
–
1476
.
60Jolly
SS
, Faxon
DP
, Fox
KA
, Afzal
R
, Boden
WE
, Widimsky
P
, Steg
PG
, Valentin
V
, Budaj
A
, Granger
CB
, Joyner
CD
, Chrolavicius
S
, Yusuf
S
, Mehta
SR
.
Efficacy and safety of fondaparinux versus enoxaparin in patients with acute coronary syndromes treated with glycoprotein IIb/IIIa inhibitors or thienopyridines: results from the OASIS 5 (Fifth Organization to Assess Strategies in Ischemic Syndromes) trial
.
J Am Coll Cardiol
2009
;
54
:
468
–
476
.
61Murphy
SA
, Gibson
CM
, Morrow
DA
, Van de Werf
F
, Menown
IB
, Goodman
SG
, Mahaffey
KW
, Cohen
M
, McCabe
CH
, Antman
EM
, Braunwald
E
.
Efficacy and safety of the low-molecular weight heparin enoxaparin compared with unfractionated heparin across the acute coronary syndrome spectrum: a meta-analysis
.
Eur Heart J
2007
;
28
:
2077
–
2086
.
62Silvain
J
, Beygui
F
, Barthelemy
O
, Pollack
C
Jr, Cohen
M
, Zeymer
U
, Huber
K
, Goldstein
P
, Cayla
G
, Collet
JP
, Vicaut
E
, Montalescot
G
.
Efficacy and safety of enoxaparin versus unfractionated heparin during percutaneous coronary intervention: systematic review and meta-analysis
.
BMJ
2012
;
344
:
e553.
63Ferguson
JJ
, Califf
RM
, Antman
EM
, Cohen
M
, Grines
CL
, Goodman
S
, Kereiakes
DJ
, Langer
A
, Mahaffey
KW
, Nessel
CC
, Armstrong
PW
, Avezum
A
, Aylward
P
, Becker
RC
, Biasucci
L
, Borzak
S
, Col
J
, Frey
MJ
, Fry
E
, Gulba
DC
, Guneri
S
, Gurfinkel
E
, Harrington
R
, Hochman
JS
, Kleiman
NS
, Leon
MB
, Lopez-Sendon
JL
, Pepine
CJ
, Ruzyllo
W
, Steinhubl
SR
, Teirstein
PS
, Toro-Figueroa
L
, White
H
.
Enoxaparin vs unfractionated heparin in high-risk patients with non-ST-segment elevation acute coronary syndromes managed with an intended early invasive strategy: primary results of the SYNERGY randomized trial
.
JAMA
2004
;
292
:
45
–
54
.
64Stone
GW
, McLaurin
BT
, Cox
DA
, Bertrand
ME
, Lincoff
AM
, Moses
JW
, White
HD
, Pocock
SJ
, Ware
JH
, Feit
F
, Colombo
A
, Aylward
PE
, Cequier
AR
, Darius
H
, Desmet
W
, Ebrahimi
R
, Hamon
M
, Rasmussen
LH
, Rupprecht
HJ
, Hoekstra
J
, Mehran
R
, Ohman
EM
.
Bivalirudin for patients with acute coronary syndromes
.
N Engl J Med
2006
;
355
:
2203
–
2216
.
65Yusuf
S
, Wittes
J
, Friedman
L.
Overview of results of randomized clinical trials in heart disease. I. Treatments following myocardial infarction
.
JAMA
1988
;
260
:
2088
–
2093
.
66Benjo
AM
, El-Hayek
GE
, Messerli
F
, DiNicolantonio
JJ
, Hong
MK
, Aziz
EF
, Herzog
E
, Tamis-Holland
JE
.
High dose statin loading prior to percutaneous coronary intervention decreases cardiovascular events: a meta-analysis of randomized controlled trials
.
Catheter Cardiovasc Interv
2015
;
85
:
53
–
60
.
67Di Sciascio
G
, Patti
G
, Pasceri
V
, Gaspardone
A
, Colonna
G
, Montinaro
A.
Efficacy of atorvastatin reload in patients on chronic statin therapy undergoing percutaneous coronary intervention: results of the ARMYDA-RECAPTURE (Atorvastatin for Reduction of Myocardial Damage During Angioplasty) Randomized Trial
.
J Am Coll Cardiol
2009
;
54
:
558
–
565
.
68Windecker
S
, Kolh
P
, Alfonso
F
, Collet
J-P
, Cremer
J
, Falk
V
, Filippatos
G
, Hamm
C
, Head
SJ
, Jueni
P
, Kappetein
AP
, Kastrati
A
, Knuuti
J
, Landmesser
U
, Laufer
G
, Neumann
F-J
, Richter
DJ
, Schauerte
P
, Uva
MS
, Stefanini
GG
, Taggart
DP
, Torracca
L
, Valgimigli
M
, Wijns
W
, Witkowski
A.
;
The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI).
2014 ESC/EACTS Guidelines on myocardial revascularization
.
Eur Heart J
2014
;
35
:
2541
–
2619
.
69Widimsky
P
, Motovska
Z
, Simek
S
, Kala
P
, Pudil
R
, Holm
F
, Petr
R
, Bilkova
D
, Skalicka
H
, Kuchynka
P
, Poloczek
M
, Miklik
R
, Maly
M
, Aschermann
M
,
Investigators P-T
.
Clopidogrel pre-treatment in stable angina: for all patients > 6 h before elective coronary angiography or only for angiographically selected patients a few minutes before PCI? A randomized multicentre trial prague-8
.
Eur Heart J
2008
;
29
:
1495
–
1503
.
70Kastrati
A
, Mehilli
J
, Schuhlen
H
, Dirschinger
J
, Dotzer
F
, ten Berg
JM
, Neumann
F
, Bollwein
H
, Volmer
C
, Gawaz
M
, Berger
PB
, Schomig
A
;
Investigators I-RS
.
A clinical trial of abciximab in elective percutaneous coronary intervention after pretreatment with clopidogrel
.
N Engl J Med
2004
;
350
:
232
–
238
.
71Schulz
S
, Mehilli
J
, Neumann
, Schuster
T
, Massberg
S
, Valina
C
, Seyfarth
M
, Pache
J
, Laugwitz
KL
, Buttner
HJ
, Ndrepepa
G
, Schomig
A
, Kastrati
A
.
ISAR-REACT 3A: a study of reduced dose of unfractionated heparin in biomarker negative patients undergoing percutaneous coronary intervention
.
Eur Heart J
2010
;
31
:
2482
–
2491
.
72Montalescot
G
, White
HD
, Gallo
R
, Cohen
M
, Steg
PG
, Aylward
PE
, Bode
C
, Chiariello
M
, King
SB
3rd, Harrington
RA
, Desmet
WJ
, Macaya
C
, Steinhubl
SR
;
STEEPLE Investigators
.
Enoxaparin versus unfractionated heparin in elective percutaneous coronary intervention
.
N Engl J Med
2006
;
355
:
1006
–
1017
.
73Schulz
S
, Mehilli
J
, Ndrepepa
G
, Neumann
FJ
, Birkmeier
KA
, Kufner
S
, Richardt
G
, Berger
PB
, Schömig
A
, Kastrati
A
.
Intracoronary Stenting and Antithrombotic Regimen: Rapid Early Action for Coronary Treatment (ISAR-REACT) 3 Trial Investigators. Bivalirudin vs. unfractionated heparin during percutaneous coronary interventions in patients with stable and unstable angina pectoris:1-year results of the ISAR-REACT 3 trial
.
Eur Heart J
2010
;
3
:
582
–
587
.
74Rose
AJ
, Allen
AL
, Minichello
T.
A call to reduce the use of bridging anticoagulation
.
Circ Cardiovasc Qual Outcomes
2016
;
9
:
64
–
67
.
75Li
Y
, Liu
Y
, Fu
L
, Mei
C
, Dai
B.
Efficacy of short-term high-dose statin in preventing contrast-induced nephropathy: a meta-analysis of seven randomized controlled trials
.
PLoS One
2012
;
7
:
e34450.
76Wang
L
, Peng
P
, Zhang
O
, Xu
X
, Yang
S
, Zhao
Y
, Zhou
Y
.
High-dose statin pretreatment decreases peri-procedural myocardial infarction and cardiovascular events in patients undergoing elective percutaneous coronary intervention: a meta-analysis of twenty-four randomized controlled trials
.
PLoS One
2014
;
9
:
e113352.
77Sardella
G
, Lucisano
L
, Mancone
M
, Conti
G
, Calcagno
S
, Stio
RE
, Pennacchi
M
, Biondi-Zoccai
G
, Canali
E
, Fedele
F
.
Comparison of high reloading rosuvastatin and atorvastatin pretreatment in patients undergoing elective PCI to reduce the incidence of myocardial peri-procedural necrosis. The ROMA II trial
.
Int J Cardiol
2013
;
168
:
3715
–
3720
.
78Fuster
V
, Chesebro
JH.
Role of platelets and platelet inhibitors in aortocoronary artery vein-graft disease
.
Circulation
1986
;
73
:
227
–
232
.
79Bybee
KA
, Powell
BD
, Valeti
U
, Rosales
AG
, Kopecky
SL
, Mullany
C
, Wright
RS
.
Pre- operative aspirin therapy is associated with improved postoperative outcomes in patients undergoing coronary artery bypass grafting
.
Circulation
2005
;
112(Suppl I)
:
I286
–
I292
.
80Paparella
D
, Brister
SJ
, Buchanan
MR.
Coagulation disorders of cardiopulmonary bypass: A review
.
Intensive Care Med
2004
;
30
:
1873
–
1881
.
81Ranucci
M
, Bozzetti
G
, Ditta
A
, Cotza
M
, Carboni
G
, Ballotta
A.
Surgical reexploration after cardiac operations: why a worse outcome?
Ann Thorac Surg
2008
;
86
:
1557
–
1562
.
82Bhaskar
B
, Dulhunty
J
, Mullany
DV
, Fraser
JF.
Impact of blood product transfusion on short and long-term survival after cardiac surgery: more evidence
.
Ann Thorac Surg
2012
;
94
:
460
–
467
.
83Jakobsen
CJ
, Ryhammer
PK
, Tang
M
, Andreasen
JJ
, Mortensen
PE.
Transfusion of blood during cardiac surgery is associated with higher long-term mortality in low-risk patients
.
Eur J Cardiothorac Surg
2012
;
42
:
114
–
120
.
84Vivacqua
A
, Koch
CG
, Yousuf
AM
, Nowicki
ER
, Houghtaling
PL
, Blackstone
EH
, Sabik
JF
3rd.
Morbidity of bleeding after cardiac surgery: is it blood transfusion, reoperation for bleeding, or both?
Ann Thorac Surg
2011
;
91
:
1780
–
1790
.
85Rossini
R
, Bramucci
E
, Castiglioni
B
, De Servi
S
, Lettieri
C
, Lettino
M
, Musumeci
G
, Visconti
LO
, Piccaluga
E
, Savonitto
S
, Trabattoni
D
, Buffoli
F
, Angiolillo
DJ
, Bovenzi
F
, Cremonesi
A
, Scherillo
M
, Guagliumi
G
;
Associazione Nazionale Medici Cardiologi Ospedalieri (ANMCO)
.
Stent coronarico e chirurgia: la gestione perioperatoria della terapia antiaggregante nel paziente portatore di stent coronarico candidato a intervento chirurgico
.
G Ital Cardiol (Rome)
2012
;
13
:
528
–
551
.
86Mangano
DT.
Multicenter Study of Perioperative Ischemia Research Group
.
Aspirin and mortality from coronary bypass surgery
.
N Engl J Med
2002
;
347
:
1309
–
1317
.
87Biondi-Zoccai
GG
, Lotrionte
M
, Agostoni
P
, Abbate
A
, Fusaro
M
, Burzotta
F
, Testa
L
, Sheiban
I
, Sangiorgi
G
.
A systematic review and meta-analysis on the hazards of discontinuing or not adhering to aspirin among 50,279 patients at risk for coronary artery disease
.
Eur Heart J
2006
;
27
:
2667
–
2674
.
88Sun
JC
, Whitlock
R
, Cheng
J
, Eikelboom
JW
, Thabane
L
, Crowther
MA
, Teoh
KH
.
The effect of pre-operative ASA on bleeding, transfusion, myocardial infarction, and mortality in coronary artery bypass surgery: a systematic review of randomized and observational studies
.
Eur Heart J
2008
;
29
:
1057
–
1071
.
89Myles
PS
, Smith
JA
, Forbes
A
, Silbert
B
, Jayarajah
M
, Painter
T
, Cooper
DJ
, Marasco
S
, McNeil
J
, Bussières
JS
, Wallace
S
;
ATACAS Investigators of the ANZCA Clinical Trials Network
.
N Engl J Med
2016
;
374
:
728
–
737
.
90Smith
PK
, Goodnough
LT
, Levy
JH
, Poston
RS
, Short
MA
, Weerakkody
GJ
, Lenarz
LA
.
Mortality benefit with prasugrel in the TRITON-TIMI 38 coronary artery bypass grafting cohort: risk-adjusted retrospective data analysis
.
J Am Coll Cardiol
2012
;
60
:
388
–
396
.
91Becker
RC
, Bassand
JP
, Budaj
A
, Wojdyla
DM
, James
SK
, Cornel
JH
, French
J
, Held
C
, Horrow
J
, Husted
S
, Lopez-Sendon
J
, Lassila
R
, Mahaffey
KW
, Storey
RF
, Harrington
RA
, Wallentin
L
.
Bleeding complications with the P2Y12 receptor antagonists clopidogrel and ticgrelor in the PLATelet inhibition and patient Outcomes (PLATO) trial
.
Eur Heart J
2011
;
32
:
2933
–
2944
.
92Varenhorst
C
, Alstrom
U
, Scirica
BM
, Hogue
CW
, Åsenblad
N
, Storey
RF
, Steg
PG
, Horrow
J
, Mahaffey
KW
, Becker
RC
, James
S
, Cannon
CP
, Brandrup-Wognsen
G
, Wallentin
L
, Held
C
.
Factors contributing to the lower mortality with ticagrelor compared with clopidogrel in patients undergoing coronary artery bypass surgery
.
J Am Coll Cardiol
2012
;
60
:
1623
–
1630
.
93Godier
A
, Taylor
G
, Gaussem
P.
Inefficacy of platelet transfusion to reverse ticagrelor
.
N Engl J Med
2015
;
372372
:
196
–
197
.
94Buchanan
A
, Newton
P
, Pehrsson
S
, Inghardt
T
, Antonsson
T
, Svensson
P
, Sjögren
T
, Öster
L
, Janefeldt
A
, Sandinge
AS
, Keyes
F
, Austin
M
, Spooner
J
, Gennemark
P
, Penney
M
, Howells
G
, Vaughan
T
, Nylander
S
.
Structural and functional characterization of a specific antidote for ticagrelor
.
Blood
2015
;
125
:
3484
–
3490
.
95Ferraris
VA
, Saha
SP
, Oestreich
JH
, Song
HK
, Rosengart
T
, Reece
TB
, Mazer
CD
, Bridges
CR
, Despotis
GJ
, Jointer
K
, Clough
ER
;
Society of Thoracic Surgeons
.
2012 update to the Society of Thoracic Surgeons guideline on use of antiplatelet drugs in patients having cardiac and noncardiac operations
.
Ann Thorac Surg
2012
;
94
:
1761
–
1781
.
96Mahla
E
, Suarez
TA
, Bliden
KP
, Rehak
P
, Metzler
H
, Sequeira
AJ
, Cho
P
, Sell
J
, Fan
J
, Antonino
MJ
, Tantry
US
, Gurbel
PA
.
Platelet function measurement-based strategy to reduce bleeding and waiting time in clopidogrel-treated patients undergoing coronary artery bypass graft surgery: the timing based on platelet function strategy to reduce clopidogrel-associated bleeding related to CABG (TARGET-CABG) study
.
Circ Cardiovasc Interv
2012
;
5
:
261
–
269
.
97Savonitto
S
, D’urbano
M
, Caracciolo
M
, Barlocco
F
, Mariani
G
, Nichelatti
M
, Klugmann
S
, De Servi
.
Urgent surgery in patients with a recently implanted coronary drug-eluting stent: a phase II study of ’bridging’ antiplatelet therapy with tirofiban during temporary withdrawal of clopidogrel
.
Br J Anaesth
2010
;
104
:
285
–
291
.
98Angiolillo
DJ
, Firstenberg
MS
, Price
MJ
, Tummala
PE
, Hutyra
M
, Welsby
IJ
, Voeltz
MD
, Chandna
H
, Ramaiah
C
, Brtko
M
, Cannon
L
, Dyke
C
, Liu
T
, Montalescot
G
, Manoukian
SV
, Prats
J
, Topol
EJ
;
BRIDGE Investigators
.
Bridging antiplatelet therapy with cangrelor in patients undergoing cardiac surgery: a randomized controlled trial
.
JAMA
2012
;
307
:
265
–
274
.
99Deo
SV
, Dunlay
SM
, Shah
IK
, Altarabsheh
SE
, Erwin
PJ
, Boilson
BA
, Park
SJ
, Joyce
LD
.
Dual anti-platelet therapy after coronary artery bypass grafting: is there any benefit? A systematic review and meta-analysis
.
J Cardiac Surg
2013
;
28
:
109
–
116
.
100Douketis
JD
, Spyropoulos
AC
, Kaatz
S
, Becker
RC
, Caprini
JA
, Dunn
AS
, Garcia
DA
, Jacobson
A
, Jaffer
AK
, Kong
DF
, Schulman
S
, Turpie
AG
, Hasselblad
V
, Ortel
T
.
Perioperative bridging anticoagulation in patients with atrial fibrillation
.
N Engl J Med
2015
;
373
:
823
–
833
.
101Hirsh
J
, Fuster
V
, Ansell
J
, Halperin
JL.
American Heart Association/American College of Cardiology Foundation Guide to Warfarin Therapy
.
Circulation
2003
;
107
:
1692
–
1711
.
102Heidbuchel
H
, Verhamme
P
, Alings
M
, Antz
M
, Diener
HC
, Hacke
W
, Oldgren
J
, Sinnaeve
P
, Camm
AJ
, Kirchhof
P
.
Updated European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist anticoagulants in patients with non-valvular atrial fibrillation
.
Europace
2015
;
17
:
1467
–
1507
.
103Beyer-Westendorf
J
, Gelbricht
V
, Forster
K
, Ebertz
F
, Köhler
C
, Werth
S
, Kuhlisch
E
, Stange
T
, Thieme
C
, Daschkow
K
, Weiss
N
.
Peri-interventional management of novel oral anticoagulants in daily care: results from the prospective Dresden NOAC registry
.
Eur Heart J
2014
;
35
:
1888
–
1896
.
104Siegal
DM
, Cuker
A.
Reversal of target-specific oral anticoagulants
.
Drug Discov Today
2014
;
19
:
1465
–
1470
.
105Pollack
CV
, Reilly
PA
, Eikelboom
J
, Glund
S
, Verhamme
P
, Bernstein
RA
, Dubiel
R
, Huisman
MV
, Hylek
EM
, Kamphuisen
PW
, Kreuzer
J
, Levy
JH
, Sellke
FW
, Stangier
J
, Steiner
T
, Wang
B
, Kam
CW
, Weitz
JI
.
Idarucizumab for Dabigatran Reversal
.
N Engl J Med
2015
;
373
:
511
–
520
.
106Siegal
DM
, Curnutte
JT
, Connolly
SJ
, Lu
G
, Conley
PB
, Wiens
BL
, Mathur
VS
, Castillo
J
, Bronson
MD
, Leeds
JM
, Mar
FA
, Gold
A
, Crowther
MA
.
Andexanet Alfa for the reversal of factor Xa inhibitor activity
.
N Engl J Med
2015
;
373
:
2413
–
2424
.
107Wiesbauer
F
, Schlager
O
, Domanovits
H
, Wildner
B
, Maurer
G
, Muellner
M
, Blessberger
H
, Schillinger
M
.
Perioperative β-blockers for preventing surgery-related mortality and morbidity: a systematic review and meta-analysis
.
Anesth Analg
2007
;
104
:
27
–
41
.
108Brinkman
W
, Herbert
MA
, Prince
SL
, Magee
MJ
, Dewey
TM
, Smith
RL
, Edgerton
JR
, Head
SJ
, Ryan
WH
, Mack
MJ
.
Preoperative β-blocker usage: is it really worthy of being a quality indicator?
Ann Thorac Surg
2011
;
92
:
788
–
796
.
109Brinkman
W
, Herbert
MA
, O’brien
S
, Filardo
G
, Prince
S
, Dewey
T
, Magee
M
, Ryan
W
, Mack
M
.
Preoperative β-blocker use in coronary artery bypass grafting surgery national database analysis
.
JAMA Intern Med
2014
;
174
:
1320
–
1327
.
110Stone
NJ
, Robinson
JG
, Lichtenstein
AH
, Bairey Merz
CN
, Blum
CB
, Eckel
RH
, Goldberg
AC
, Gordon
D
, Levy
D
, Lloyd-Jones
DM
, McBride
P
, Schwartz
JS
, Shero
ST
, Smith
SC
Jr, Watson
K
, Wilson
PW
, Eddleman
KM
, Jarrett
NM
, LaBresh
K
, Nevo
L
, Wnek
J
, Anderson
JL
, Halperin
JL
, Albert
NM
, Bozkurt
B
, Brindis
RG
, Curtis
LH
, DeMets
D
, Hochman
JS
, Kovacs
RJ
, Ohman
EM
, Pressler
SJ
, Sellke
FW
, Shen
WK
, Smith
SC
Jr, Tomaselli
GF
;
American College of Cardiology/American Heart Association Task Force on Practice Guidelines
.
2013 ACC/AHA Guideline on the treatmentof blood cholesterol to reduce atherosclerotic cardiovascular risk in adults
.
Circulation
2014
;
129(Suppl 2)
:
S1
–
S45
.
111Kulik
A
, Ruel
M
, Jneid
H
, Ferguson
TB
, Hiratzka
LF
, Ikonomidis
JS
, Lopez-Jimenez
F
, McNallan
SM
, Patel
M
, Roger
VL
, Sellke
FW
, Sica
DA
, Zimmerman
L
;
American Heart Association Council on Cardiovascular Surgery and Anesthesia
.
Secondary prevention after coronary artery bypass graft surgery: a scientific statement from the American Heart Association
.
Circulation
2015
;
131
:
927
–
964
.
112Kulik
A
, Brookhart
MA
, Levin
R
, Ruel
M
, Solomon
DH
, Choudhry
NK.
Impact of statin use on outcomes after coronary artery bypass graft surgery
.
Circulation
2008
;
118
:
1785
–
1792
.
113Kuhn
EW
, Slottosch
I
, Wahlers
T
, Liakopoulos
OJ.
Preoperative statin therapy for patients undergoing cardiac surgery
.
Cochrane Database Syst Rev
2015
;
8
:
CD008493
.
© The Author 2017. Published on behalf of the European Society of Cardiology.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/), which permits non-commercial re-use, distribution, and reproduction in any medium, provided the original work is properly cited. For commercial re-use, please contact
[email protected]











{kind=link}