




Abstract
A 20 years old boxer had undergone usual sport medicine examination complaining palpitations and some ventricular premature beats (PVC) were documented at ECG. He had no remarkable past medical history except for known right bundle branch block (RBBB) and bicuspid heart valve with minimum valve regurgitation but no aortic dilation. He showed up in our arrhythmia clinic. The 12 leads, 24 hours ECG Holter showed very high PVC burden (58000, 51% of overall beats), including some non sustained ventricular tachycardia. PVC morphology was monomorphic (fig.1), RBBB pattern, V1 transition, inferior axis, negative wave in I lead, pseudo–delta wave, QS in the most negative lead aVL corresponding to lateral left ventricular summit (LVS). Transthoracic echocardiogram and ergonometric test documented no relevant finds. Due to PVC morphology, MRI was carried out documenting mid lateral subtle area of sub–epicardial late gadolinium enhancement (LGE), but normal bi–ventricular function, suggesting idiopathic PVC in a patient with structural heart disease. Anti–arrhythmic therapy failed so we decided to pursue catheter ablation. However, LVS ablation is complex due to epicardial location and the presence of coronary vessels, so we performed an heart CT scan to merge it with electro–anatomical mapping (EAM). Vantage point ablation strategy was chosen. First of all we performed right ventricle outflow tract (RVOT) mapping: pace mapping was not so good, but we found an early as much as rounded EGM during PVC (fig. 2). Then, we mapped coronary venous system identifing a sharp and early EGM (fig. 2) as good pace mapping in the great cardiac vein, where we started ablation. CT was fundamental to keep the right distance from inter ventricular artery. PVC burden was not abolished so we unsuccessfully tried to ablate RVOT site (fig. 3). Finally, by retrograde approach via femoral artery, we reached left ventricular outflow tract finding the earliest site of activation near left main (fig. 3), CT and EAM merge help to control distance (fig. 3), so we safely ablated it obtaining PVC disappearance, also during isoproterenol infusion. During long term follow up, the patient remained asymptomatic and no further PVC have been recorded. Due to the presence of LGE at cardiac MRI, regular follow up will be continue. LVS ablation can be often approached by sequential ablation of the surrounding structures and heart CT scan merging with EAM improving the success rate and the safety.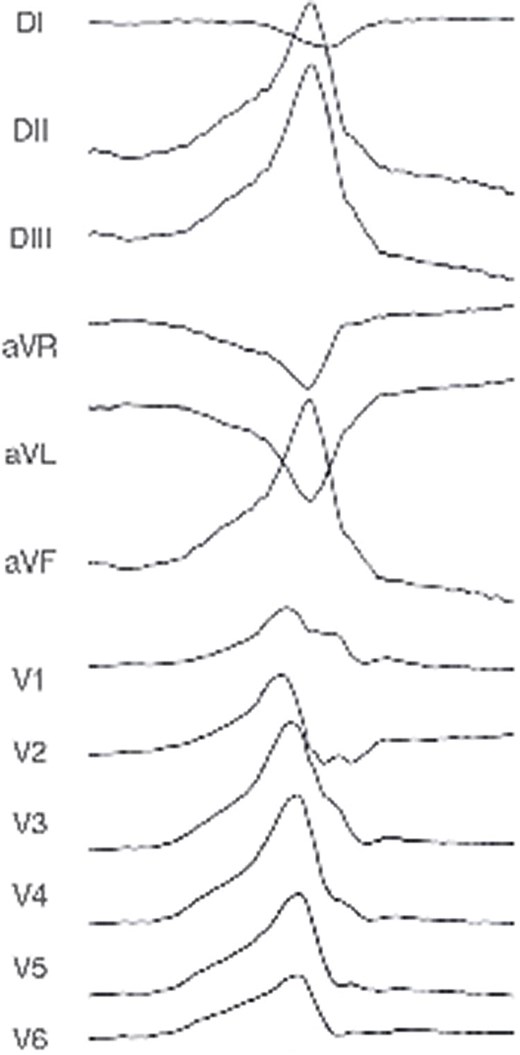
Figure 1

Figure 2
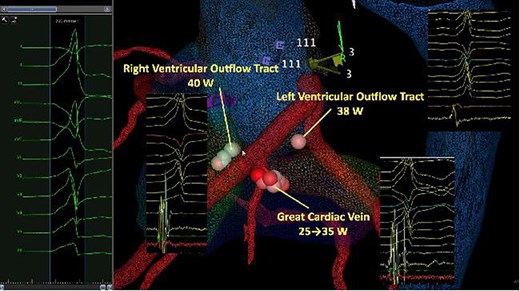
Figure 3
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Society of Cardiology. All rights reserved. For commercial re-use, please contact [email protected] for reprints and translation rights for reprints. All other permissions can be obtained through our RightsLink service via the Permissions link on the article page on our site—for further information please contact [email protected].
This article is published and distributed under the terms of the Oxford University Press, Standard Journals Publication Model (https://dbpia.nl.go.kr/pages/standard-publication-reuse-rights)



{kind=link}
{kind=link}
{kind=link}