




Cover image
Cardiac tamponade after pulmonary endarterectomy: mind the left side…
Lior Bibas1, Moza Al-Kalbani1, Marc de Perrot2, and Ghislaine Douflé1,3*
1Interdepartmental Division of Critical Care Medicine, University of Toronto, Toronto General Hospital, University Health Network, 200 Elizabeth Street, Toronto, Ontario M5G 2C4, Canada; 2Division of Thoracic Surgery, Toronto General Hospital, University Health Network, 200 Elizabeth Street, Toronto, Ontario M5G 2C4, Canada; and 3Department of Anesthesia, Toronto General Hospital, University Health Network, 200 Elizabeth Street, Toronto, Ontario M5G 2C4, Canada
*Corresponding author. Tel: 11 416 340 4645, Email: [email protected]
Two of our patients presented cardiac tamponade post-surgical pulmonary endarterectomy for chronic thromboembolic pulmonary hypertension (CTEPH). Both patients were therapeutically anticoagulated and presented with refractory shock on post-operative Day 4 (Patient A) and Day 10 (Patient B), respectively. Echocardiograms did not demonstrate classical right-sided chamber collapse albeit demonstrated moderate to large pericardial effusion with frank diastolic collapse of the left ventricle and impeded filling. Both patients received a therapeutic pericardiocentesis; Patient A underwent thoracotomy for surgical exploration and pericardial evacuation, whereas Patient B underwent a bedside ultrasound-guided pericardiocentesis. Pericardial drainage led to marked haemodynamic improvement.
Pericardial tamponade after pulmonary endarterectomy is a rare but life-threatening surgical complication. Patients with CTEPH are usually anticoagulated early in their post-operative course. Presence of right ventricular hypertrophy may protect the right ventricle from increased intrapericardial pressures, which explains why both our patients exhibited left ventricular collapse preceding right chamber collapse in the context of a new, large circumferential pericardial effusion.
It is important to keep a high index of suspicion for cardiac tamponade in haemodynamically unstable patients after pulmonary endarterectomy, which may appear days or weeks after surgery. While ultrasound remains an important tool in the evaluation and management of post-operative pericardial effusion, cardiac tamponade remains a clinical diagnosis, as classic echocardiographic signs may be absent (especially when mechanically ventilated). Furthermore, patients with chronic pulmonary hypertension and right ventricular hypertrophy, present additional challenge as left-sided chamber collapse may occur first.
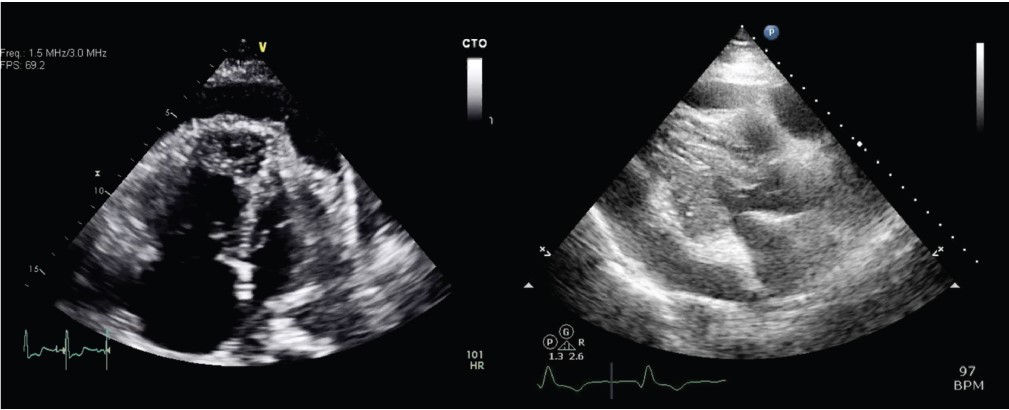
Panel 1 (left: patient A): apical four-chamber view showing a large pericardial effusion with diastolic collapse of the apical left ventricular wall. Panel 2 (right: patient B): parasternal long-axis view demonstrating a large pericardial effusion with diastolic collapse of the mid-infero-lateral left ventricular wall.
Supplementary material is available at European Heart Journal online.
Volume 40, Issue 19, 14 May 2019
Focus Issue on NOACs
Issue @ A Glance
Unresolved issues of anticoagulation in atrial fibrillation: age, BMI, reduced dose, and ethnicity
CardioPulse
Breaking Down the Hierarchy of Medicine: The airline industry has taken the lead to improve communications for pilots, it is now time for medicine to follow with physicians
Biomarkers and Cardiovascular Risk Stratification: Extensive research reports that biomarkers may be helpful in the assessment of thromboembolic and bleeding risk in patients with atrial fibrillation. At the same time, increasing evidence suggests their role in personalized medicine and in prediction of clinical outcomes in heart failure
Impact of the New ACC/AHA and ESC/ESH Hypertension Guidelines for Norway
Acute Coronary Syndromes in Cancer Patients: The differences of ACS in cancer patients and the general population are discussed
Dr Aram J. Mirza and cardiology in Kurdistan: First TAVI at the Slemani Cardiac Hospital in Kurdistan and a vision towards a Center of excellence in cardiovascular medicine in Kurdistan, Iraq and the Middle-East
Clinical Research
Atrial fibrillation
Efficacy and safety of reduced-dose non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation: a meta-analysis of randomized controlled trials

Editorial
On-label reduced doses of non-vitamin K anticoagulants prove safe and efficient; yet how to ensure the correct dose for the right patient?

Age threshold for the use of non-vitamin K antagonist oral anticoagulants for stroke prevention in patients with atrial fibrillation: insights into the optimal assessment of age and incident comorbidities

Editorial
Fine-tuning the decision to initiate anticoagulation in atrial fibrillation by accounting for age and cardiovascular comorbidities
Clinical outcomes, edoxaban concentration, and anti-factor Xa activity of Asian patients with atrial fibrillation compared with non-Asians in the ENGAGE AF-TIMI 48 trial
Editorial
Stroke prevention in AF: Of Asians and non-Asians
When is it appropriate to stop non-vitamin K antagonist oral anticoagulants before catheter ablation of atrial fibrillation? A multicentre prospective randomized study

Editorial
Saving the brain from catheter ablation of atrial fibrillation: the role of pre- and peri-procedural anticoagulation

Thrombosis and antithrombotic therapy
Relationship between body mass index and outcomes in patients with atrial fibrillation treated with edoxaban or warfarin in the ENGAGE AF-TIMI 48 trial

Editorial
The evolving obesity paradigm story: from heart failure to atrial fibrillation
Dabigatran dual therapy with ticagrelor or clopidogrel after percutaneous coronary intervention in atrial fibrillation patients with or without acute coronary syndrome: a subgroup analysis from the RE-DUAL PCI trial


