




Cover image
Chronic pararenal aortic and iliac occlusion
Mattia Cattaneo1,2*, Carla Puligheddu3, Gabutti Luca2,4, and Augusto Gallino1,5
1Department of Cardiovascular Medicine, Ospedale Regionale di Bellinzona e Valli – San Giovanni, Via Ospedale, 6500 Bellinzona, Switzerland; 2Department of Internal Medicine, Ospedale Regionale di Bellinzona e Valli – San Giovanni, Via Ospedale, 6500 Bellinzona, Switzerland; 3Department of Radiology, Ospedale Regionale di Bellinzona e Valli – San Giovanni, Via Ospedale, 6500 Bellinzona, Switzerland; 4University of Lausanne, Lausanne, Switzerland; and 5University of Zurich, Zurich, Switzerland
*Corresponding author. Tel: +41 91 811 85 34, Fax +41 91 811 91 69, Email: [email protected]
A 76-year old deaf-dumb man known for metabolic syndrome, cerebrovascular disease, worsening renal function, a 40 pack year smoking history, and alcohol abuse was admitted for an uncomplicated head trauma after an accidental fall. Medical history was significant for a IIb stage Fontaine (Rutherford 2 stage) claudication. Physical examination showed neither abdominal bruits nor ischaemic changes of skin and subcutaneous tissues of the lower limbs (LL). There was a bilateral severe reduction of the ankle–brachial index, thus diagnosing significant LL peripheral artery disease.
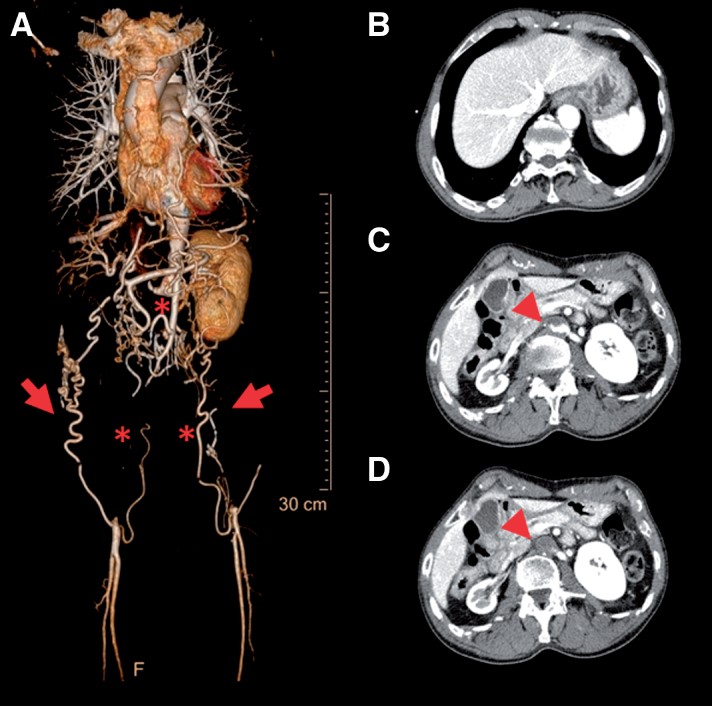
The patient underwent a computed tomography angiography that disclosed a complete chronic thrombotic occlusion of the pararenal abdominal aorta (AA) and bilateral aortoiliac occlusion including the entire external iliac arteries (Panel A, *). Common femoral arteries were perfused bilaterally by collaterals. Systemic collateral pathways from the abdominal wall (Panel A, red arrows) connected the superior and inferior circulations. Right renal artery was included in the atherothrombotic occlusion with complete occlusion and ipsilateral renal atrophy (Panels C and D, red arrows). Subsequently, to his comorbidities, the alcohol abuse and the fragile social environment, it was decided to pursue a conservative management by best medical therapy. Chronic occlusive disease represents a minority of patients with aortoiliac disease.
This case involving the pararenal AA, renal, and complete bilateral iliac arteries chronic occlusion represents an unusual and severe manifestation in this group. Chronic occlusion still embodies a complex management and treatment issue. Medical, endovascular, and surgical management have been proposed, however, the management should be individualized.
Volume 39, Issue 47, 14 December 2018
Issue @ A Glance
Arterial and pulmonary hypertension: risk assessment and current pharmacological and interventional management
CardioPulse
Named lectures at ESC Congress 2018
Appropriate use criteria adoption for PCI at an academic medical center
FIFA World Cup 2018
Professor Sanjay Sharma FESC
Viewpoint
Catheter-based renal denervation: the next chapter begins
Clinical Review
Prevention and epidemiology
Epigenetics and precision medicine in cardiovascular patients: from basic concepts to the clinical arena
Clinical Research
Differential impact of syncope on the prognosis of patients with acute pulmonary embolism: a systematic review and meta-analysis
Hypertension
Asleep blood pressure: significant prognostic marker of vascular risk and therapeutic target for prevention
Editorial
Asleep blood pressure: a target for cardiovascular event reduction?

Pulmonary arterial hypertension
A comprehensive risk stratification at early follow-up determines prognosis in pulmonary arterial hypertension
Editorial
Validation of a risk assessment instrument for pulmonary arterial hypertension
Pulmonary circulation
Outcomes after extracorporeal membrane oxygenation for the treatment of high-risk pulmonary embolism: a multicentre series of 52 cases
Editorial
Extracorporeal cardiopulmonary support in acute high-risk pulmonary embolism: still waiting for solid evidence


