





Abstract
Anthracycline-based chemotherapy has improved the prognosis in cancer and hematological malignancies but is associated with the development of heart failure (HF). Besides well-known cardiac risk factors and cumulative dose of anthracycline, recent research has suggested that genetic variations associated with cardiomyopathies may increase the risk of HF associated with anthracycline. However, the importance of familial predisposition for the risk of developing anthracycline associated cardiotoxicity is unknown.
To evaluate the risk of anthracycline related HF in patients with vs. without a first-degree relative with HF.
In the nationwide Danish registries, patients treated with anthracycline from 2004–2016 were identified. Primary outcome was a subsequent diagnosis of HF. Follow-up was 10 years or December 31, 2017. Familial relations were identified in the Danish Family Registry, which hold all persons born since 1942. Exposure was a first-degree biological relative (parent or sibling) with a diagnosis of HF. Risk of HF was evaluated in a cumulative incidence function with death as competing event and in a Fine and Grey model adjusted for age, sex, prevalent ischemic heart disease, atrial fibrillation, hypertension and chronic obstructive pulmonary disease.
A total of 11.651 patients (mean age 48.0 (SD±8.6), 12.2% male gender) were evaluated after exclusion of 46 with pre-anthracycline HF. Mean follow-up was 4.4 years (SD±2.9). In the group with a first-degree relative with HF (n=1.608) 35 patients (2.2%) was diagnosed with HF vs. 133 (1.3%) in the group without a first-degree relative with HF (n=10.043) corresponding to incidence rates per 1000 patient years of 5.2 (95% CI: 3.8–7.3) vs. 3.0 (95% CI: 2.5–3.5). The cumulative incidence of HF was higher in the first-degree relative HF group (Figure 1a), yielding an adjusted hazard ratio of 1.53 (95% CI: 1.05–2.24, p=0.03) for HF associated with anthracycline. All-cause mortality showed a trend towards higher risk in the later 5 years of follow-up in the first-degree relative HF group with a 10-year risk of 32.4% (95% CI: 28.4–36.5) vs. 26.1% (95% CI: 24.9–27.4) but no significant difference in the Kaplan-Meier estimate (p=0.08) (Figure 1b).
In this nationwide register-based study having a first-degree relative with HF was associated with a small but increased risk of anthracycline related HF, yielding attention towards the family predisposition, when estimating the risk of cancer therapy related cardiotoxicity.
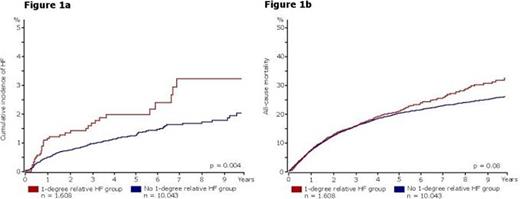
Figure 1
Type of funding source: Public hospital(s). Main funding source(s): Odense University Hospital


{kind=link}