





Abstract
Guidelines favor patient selection by left bundle branch block (LBBB) with QRS width ≥150 ms for cardiac resynchronization therapy (CRT). However, predicting response to CRT patients with QRS width 120 to 149 ms or non-LBBB remains difficult. Speckle tracking left atrial (LA) strain is a novel means to assess cardiac function, however its applications to CRT patients remains unclear.
To test the hypothesis that baseline LA strain has prognostic value in CRT patients with intermediate ECG criteria.
We studied 195 patients with heart failure (HF) who underwent CRT based on routine indications: ejection fraction ≤35% and QRS width ≥120 ms. GLS was assessed using the 3 standard apical views. LA longitudinal strain was based on 12 segments from the 2 and 4-chamber apical view. Peak LA strain, a measure associated with the reservoir function of the LA, was defined as the average of peak longitudinal strain from all segments. The predefined combined clinical endpoint was death, heart transplant or left ventricular assist device (LVAD) over 4 years after CRT.
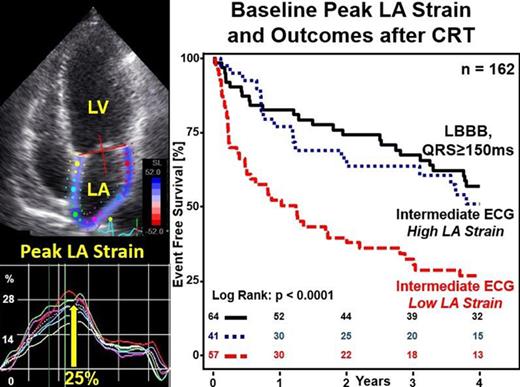
LA strain was feasible in 162 (83%) of the candidates for CRT: age 64±11 years, 72% male, QRS duration 156±26 ms, 39.5% had LBBB with QRS ≥150ms, 60.5% had intermediate ECG criteria. Median LA strain was 11.0% [1.3% - 36.8%]. High LA peak strain was associated with more favorable event-free survival and Low LA Peak strain was associated with worse clinical outcome following CRT (FIGURE, p<0.001). Patients with intermediate ECG criteria for CRT (non-LBBB or QRS width 120 to 149 ms) and high peak LA strain had similar outcome to those with Class I indications for CRT (LBBB and QRS≥150 ms). Multivariable analysis revealed that LA strain had independent prognostic value (hazard ratio 0.98 per LA strain %, p<0.01) even after adjusted for other clinical, electrophysiological and echocardiographic covariates including QRS morphology and duration, ischemic cardiomyopathy, LVEF and global longitudinal strain.
Baseline peak LA strain had important prognostic value in HF patients who are candidates for CRT. Prognostic value of LA strain was most significant in CRT patients with intermediate ECG criteria (QRS 120 to 149ms or non-LBBB) and has promise for clinical applications.
LA strain and clinical outcome after CRT
Type of funding source: None


{kind=link}