





Abstract
The number of cancer patients with known cardiovascular (CV) disease is increasing due to improved cancer prognosis.
The objective of this study is to assess the long-term results of cancer patients referred to a cardiology department by primary care using electronic consultation (e-consultation).
We analysed the patients with previous diagnosis of cancer referred to a cardiology department (CD) from 2010 to 2021 (n=6.889), selected from a total of 68.518 patients (61.629 without cancer), and compared two assistance models: in-person practice (from 2010 to 2012) and e-consultation (from 2013 to 2021). In the first period, all the patients referred by primary care physicians (PCPs) were seen in an in-person consultation and in the e-consultation model the cardiologist reviewed the electronic records (e-consultation) and decided to solve without any visit or, if it was necessary, with an in-person consultation. The outcomes between both periods were analysed using an interrupted time series regression model: 1) delay time to cardiology assistance; 2) all-cause and cardiovascular hospital admissions, and 3) all-cause and cardiovascular mortality during the first year after the initial consultation or e-consultation to the CD.
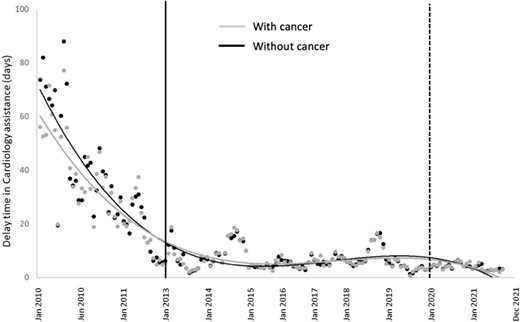
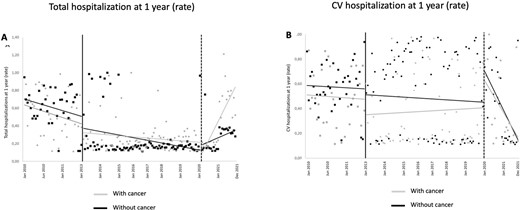
Among cancer patients referred to cardiology consultation, the introduction of e-consultation decreased waiting times to cardiology care by 51,8% (95% CI: 51,7%-51,9%) (Fig 1). Over 60% of referrals were resolved in less than 8 days, with this proportion significantly higher after the e-consultation program was introduced (p<0,001). Furthermore, we observed a reduction in the one-year rate of outcomes, with an incidence rate ratio (iRR) [IC 95%] of 0,75 [0,73-0,77] for CV-related hospitalizations (Fig 2b), 0,43 [0,42-0,44] for all-cause hospitalization (Fig 2a), and 0,87 [0,86-0,88] for all-cause mortality. In the multivariate analysis, the delay in receiving cardiology care was significantly associated with an independent increase in 1-year mortality (OR [95% CI] 1,39 [1,06-1,83]) and hospital admission (OR [95% CI] 1,25 [1,02-1,52]). Furthermore, the implementation of the e-consult model was associated with a reduction in hospital admission rates (OR [95% CI] 0,19 [0,14-0,25]).
Author notes
Funding Acknowledgements: None.


{kind=link}