





Abstract
PMI are characterized by an elevation in cardiac biomarkers, such as troponin, following PCI. Adherence to the 4th UDMIof PMI necessitates not only elevated cardiac biomarkers but also the presence of ECG changes, new loss of viable myocardium, or angiographic findings indicative of a procedural complication. Understanding the mechanisms underlying PMI and their associated factors is of paramount clinical significance. Our goal was to investigate the specific pathways contributing to the occurrence of PMI in stable patients undergoing PCI.
This prospective study was performed at 23 sites and enrolled patients with at least one epicardial lesion with an FFR≤0.80 planned to be treated by PCI. Each patient underwent a standardized physiological protocol, including manual FFR pullbacks with PPG calculation for the characterization of CAD patterns. The median PPG value (0.62) was used to divide patients into predominantly focal or diffuse disease. Troponin levels were measured after PCI, and patients exhibiting an elevation exceeding 5 times the upper limit of normal (ULN) were subject to evaluation by an independent clinical events committee. In addition, patients with large troponin elevation (>70 times above the ULN) were adjudicated as PMI as a standalone criterion. The primary objective was to investigate the mechanism leading to PMI in patients with focal versus diffuse CAD.
Overall, 855 patients were included in this analysis, with 34.5% (295 patients) exhibiting a troponin elevation exceeding 5 times the ULN. Among these cases, 66 (7.7%) were adjudicated as PMI. The prevalence of secondary criteria for PMI was as follows: ECG changes at 7.6% (5/66), new loss of viable myocardium at 0%, side branch occlusion at 18.2% (12/66), and large troponin elevation at 84.8% (56/66). Diffuse disease (PPG < 0.62) was significantly associated with PMI (OR 1.71, 95% CI 1.03 to 2.88, p-value = 0.038). In the overall population, the occurrence of ECG changes after PCI was 0.7% in focal disease compared to 0.8% in diffuse disease (p-value=1.0). Side branch occlusion after PCI was observed in 0.7% in focal disease vs. 2.5% in diffuse disease (p-value=0.04), and large troponin elevation occurred in 4.8% in focal disease vs. 8.5% in diffuse disease (p-value=0.03). Additionally, PPG was significantly associated with the incidence of side branch occlusion (OR 1.71, 95% CI 1.03 to 2.88, p-value=0.038) and large troponin elevation after PCI (OR 1.83, 95% CI 1.06 to 3.22, p-value=0.038).
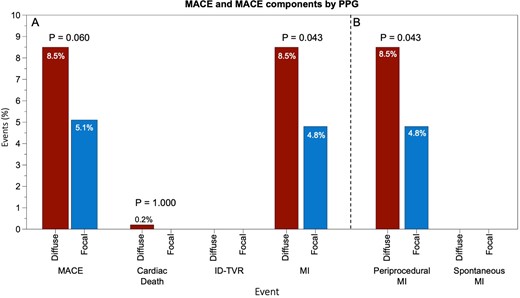
MACE by PPG
Author notes
Funding Acknowledgements: Type of funding sources: Private grant(s) and/or Sponsorship. Main funding source(s): The study was sponsored by the Cardiovascular Research Institute (CRI) Aalst with an unrestricted grant from Abbott Vascular.


{kind=link}