





Abstract
Sudden cardiac death (SCD) in patients with ischemic cardiomyopathy (ICM) remains a leading cause of death. Current guidelines provide a class I recommendation for implantable cardioverter–defibrillator (ICD) implantation in ICM patients with transthoracic echocardiographic (TTE) left ventricular ejection fraction (LVEF) ≤35%. and NYHA functional class II or III. The current paradigm is suboptimal in identifying patients who are likely to benefit. In fact, only a relatively small proportion of ICD recipients for SCD primary prevention receive appropriate device therapy and instead there is a not negligible percentage of patients who experienced SCD event despite not fulfilling criteria for implantation.
The DERIVATE-ICM registry sought to evaluate the additional prognostic value for the indication of ICD implantation using cardiac magnetic resonance (CMR) as compared to standard of care based on TTE in a large cohort of ICM patients.
We enrolled 861 ICM patients (86% male, mean age 65±11 years) with chronic heart failure and TTE-LVEF<50%. Major adverse arrhythmic cardiac events (MAACE), defined as the combination of SCD, aborted SCD event, and sustained ventricular tachycardia. were the primary endpoint. Independent predictors were used to calculate a CMR risk score for each patient. Risk levels were defined as low (quantile 1 [Q1]), medium (Q2 and Q3) and high (Q4).
During a median follow-up of 1054 days, MAACE occurred in 88 (10.2%). Left ventricular end-diastolic volume index (HR:1.007, 95%CI:1.000-1.011, p=0.05), CMR-LVEF (HR:0.972, 95%CI: 0.945-0.999, p=0.045) and late gadolinium enhancement (LGE) mass (HR:1.010, 95%CI: 1.002–1.018, p=0.015) were independent predictors of MAACE. Based on the multivariate analysis, CMR weighted risk score was developed according to the following equation [0.005 * EDV/BSA (mL/m2) – 0.029 * LVEF (%) + 0.010 * LGE ischemic mass (g)]. A multiparametric CMR weighted predictive derived score effectively identifies subjects at high risk for MAACE as compared to TTE-LVEF cut-off of 35% with a Continuous NRI: 31.7% (95%CI: 8.6%-54.8%, p=0.007) (Figure 1, Figure 2).
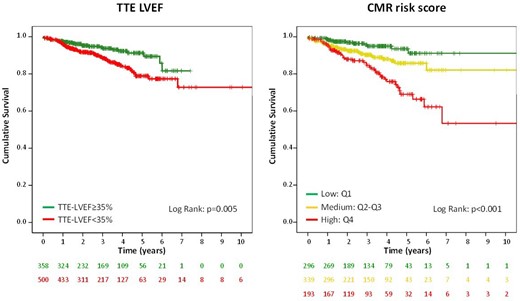
Kaplan-Meier curves
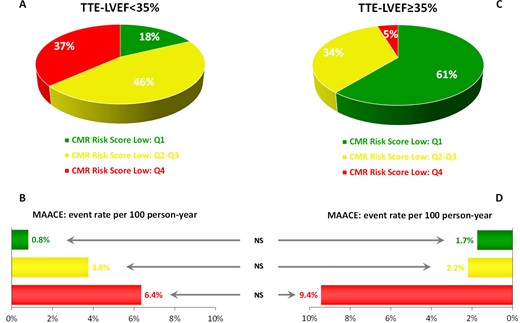
Event rate redistribution
Author notes
Funding Acknowledgements: Type of funding sources: Public Institution(s). Main funding source(s): This work was supported by Italian Ministry of Health, Rome, Italy.


{kind=link}