





Abstract
Cardiac amyloidosis (CA) is a rapidly progressive disease that portends poor prognosis. Recently, transthyretin-derived CA (ATTR-CA) has attracted attention due to the emergence of specific drugs, and its simple and accurate diagnosis is required. Apical sparing pattern of regional longitudinal strain (LS) distribution has been known as specific echocardiographic finding for CA. However, its diagnostic significance is unclear when limited to ATTR-CA.
This study aimed to investigate the diagnostic accuracy of apical sparing pattern to distinguish ATTR-CA from other left ventricular hypertrophic diseases.
This was a retrospective study evaluating 32 patients underwent endomyocardial biopsy for differentiation of left ventricular hypertrophy from November 2018 to August 2022. Based on clinical data, patients were classified into 9 patients in ATTR-CA, 14 patients in hypertrophic cardiomyopathy (HCM), and 9 patients in hypertensive heart disease (HHD). In addition to routine echocardiographic findings, left ventricular LS analysis was performed. Relative regional strain ratio (RRSR) as an index of apical sparing pattern was measured as the average of apical LS divided by the sum of the average of mid and basal LS values.
RRSR in ATTR-CA group was significantly higher than in HCM and HHD groups (0.96 vs. 0.68 vs. 0.72, P=0.004) (Table). In the receiver-operating characteristic analysis of RRSR for differentiating ATTR-CA from HCM and HHD, the optimal cut-off value of RRSR for the diagnosis of ATTR-CA was 0.93 (sensitivity 67%, specificity 96%, area under the curve 0.84) (Figure).
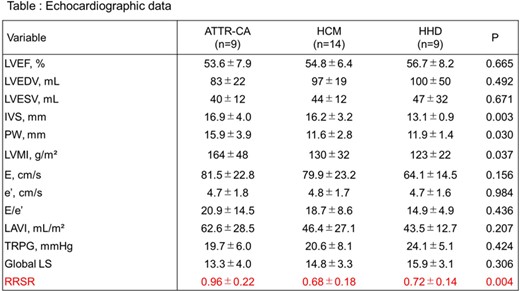
Echocardiographic data

Author notes
Funding Acknowledgements: None.


{kind=link}