





Abstract
Type of funding sources: None.
Patients with secondary tricuspid regurgitation (TR) represent a heterogeneous group that benefits differentially from tricuspid annuloplasty. We hypothesized that TR severity may be proportional or disproportional to right ventricular (RV) remodeling and investigated the prognostic implications of this novel paradigm.
The ratios of pre-procedural effective regurgitant orifice area (EROA) with right ventricular end-diastolic area (RVDA) and tricuspid annular plane systolic excursion (TAPSE) were retrospectively assessed in 307 patients undergoing tricuspid annuloplasty. Based on optimal thresholds derived from cubic splines and maximally selected rank statistics, patients were stratified into 3 groups: proportionate TR (Group 1: EROA/RVDA ≤1.68 and EROA/TAPSE ≤3.42), disproportionate TR to RV size (Group 2: EROA/RVDA >1.68 and EROA/TAPSE ≤3.42), and disproportionate TR to RV size and function (Group 3: EROA/RVDA >1.68 and EROA/TAPSE >3.42).
Overall, 72 (23%), 127 (41%), and 108 (35%) patients were classified into Group 1, 2, and 3, respectively. Compared with those with proportionate TR (Group 1), patients with disproportionate TR (Group 2 and 3) had a higher prevalence of atrial fibrillation, moderate to severe aortic stenosis, and smaller left ventricular end-diastolic and end-systolic volumes. During a median (interquartile range) follow-up of 4.3 (2.6-6.3) years, 74 adverse events (42 HF hospitalizations and 32 deaths) occurred. Patients with disproportionate TR (Group 2 and 3) had higher rates of adverse events than those with proportionate TR (21% and 38% versus 8%; P = 0.010 and P < 0.001, respectively; Figure) and were independently associated with poor outcomes on multivariate analysis. Importantly, this novel framework outperformed the TR grading system recommended by current guidelines, which was unable to effectively stratify prognosis in this population (Hazard Ratio for severe versus moderate TR 1.42; 95% CI 0.84-2.38; P = 0.194).
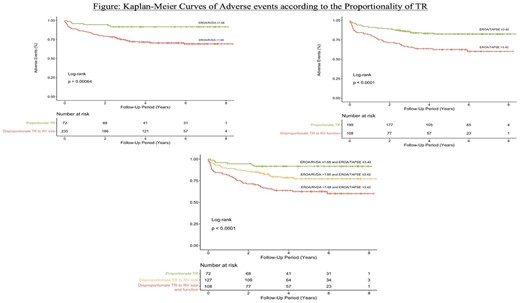
Abstract Figure.


{kind=link}