





Abstract
Type of funding sources: None.
Primary percutaneous intervention remains the principal treatment modality for anterior wall myocardial infarction (AWMI). However, a large fraction of patients especially in the developing countries present outside the window period (OWP) with no chest pain and akinetic left anterior descending (LAD) territory on echocardiography. Revascularization in these patients is primarily guided by viability status.
This study was conducted to determine the accuracy of strain echocardiographic parameters compared to single-photon emission computed tomography (SPECT) in predicting myocardial viability in patients of AWMI presenting OWP.
All patients presenting with AWMI-OWP without ongoing chest pain and akinetic LAD territory on echocardiography from December 2020 to June 2021 were recruited. All patients underwent determination of both Global longitudinal strain (GLS) and territorial longitudinal strain (TLS) within 24-72 hours on AWMI. In addition, all underwent SPECT to determine the percentage of non-viable myocardium. On SPECT, a defect >5% myocardial territory showing severe reperfusion defect was considered as a marker of non-viability.
A total of 27 patients were recruited. The mean age of the population was 61.66 + 12.6 years. Acute left ventricular failure (LVF) and cardiogenic shock (CS) was present in 6 (22.2%) and 5 (18.5%) patients respectively. Out of 22 patients who underwent angiography, majority of the patients 19 (86%) had single vessel disease involving the LAD.
The mean left ventricular ejection fraction (LVEF) of the study group was 29.6 + 6.5%. The mean GLS and LAD territory TLS of the study group was -11.13 + 3.14% and -7.2 + 2.75% respectively. On SPECT, 8 (29.6%) patients had non-viable underlying myocardium.
Parameters that very significantly associated with non-viability on SPECT included past history of CAD (p = 0.004), smoking (p = 0.05) and presentation with LVF (p = 0.0008) and CS (p = 0.001).
The mean LVEF was significantly lower in the group with non-viability on SPECT (32.3 + 5.1% vs 23.1 + 4.5%; p < 0.001). Both GLS (-12.8 + 1.4% vs -7.1+ 2.3%; p < 0.001) and TLS (-8.7 + 1.4% vs -3.8 + 1.8%; p < 0.001) were significantly lower in group showing non-viability on SPECT.
On receiver operating curves, a GLS of > -10.45% and TLS of > -6.65%, both had a sensitivity of 87.5% and specificity of 89.5% in predicting non-viability on SPECT. Both showed good accuracy in predicting non-viability on overall quality model. (Figures 1 and 2)
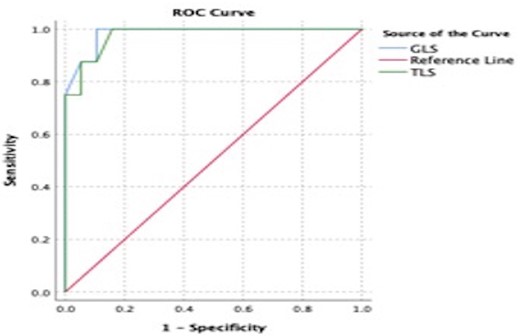
Abstract Figure.
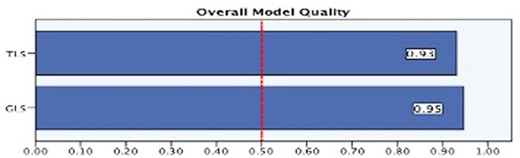
Abstract Figure. Overall quality model


{kind=link}