





Abstract
Several ECG signs have been proposed to discern the focal origin of ventricular outflow tract arrhythmias with a transition ≥V3. Their independent predictive value is unclear.
The aim of the study is to establish a predictive model of independent ECG parameters to obtain an acute success in right-sided catheter ablation of isolated premature ventricular contractions (PVCs) or ventricular tachycardia (VT) from the ventricular outflow tract with a transition ≥V3.
We included 122 patients (62 women, mean age 54±16 years) with documented PVCs or VT showing a lower axis and predominantly negative QRS complexes in V1 and V2 who underwent ablation between January 2014 and June 2020. The achievement of acute ablation success from right endocardial positions was assessed. We performed a predictive model by multivariate logistic regression analysis including the following ECG variables associated with a right origin of the ventricular focus in previous studies: Transitional Zone (TZ) index, V2 transition ratio, V2S / V3R index, R-wave duration index, R/S-wave amplitude index in V2, variable coupling interval, and the presence of QS morphology in lead I.
Two independent predictive ECG variables were identified: the V2S / V3R index (odds ratio 1.223; 95% CI, 1.024–1.460; p=0.026) and a coupling interval variability >60 ms (odds ratio 0.307; 95% CI, 0.129 - 0.731; p=0.008). The area under the curve of this model was 0.733 (Picture 1). Arrhythmias with transition in V3 present a greater electroanatomic overlap and, therefore, a higher probability of right failure (59.3% vs 73.5% in arrhythmias with transitions after V3). In these, the V2 transition ratio is useful to predict the origin of the ectopy.
Two easily identifiable ECG variables (the V2S / V3R index and coupling interval variability >60 ms) predict the acute success of a right-sided approach in the ablation of focal ventricular arrhythmias with predominantly negative QRS complexes in V1 and V2.
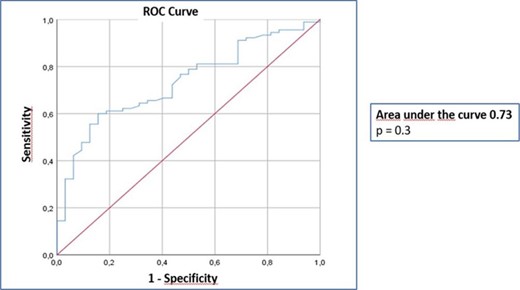
Predictive accuracy of the ECG model


{kind=link}