





Abstract
This review covers the last 80 years of remarkable progress in the development of mineralocorticoid receptor (MR) antagonists (MRAs) from synthesis of the first mineralocorticoid to trials of nonsteroidal MRAs. The MR is a nuclear receptor expressed in many tissues/cell types including the kidney, heart, immune cells, and fibroblasts. The MR directly affects target gene expression—primarily fluid, electrolyte and haemodynamic homeostasis, and also, but less appreciated, tissue remodelling. Pathophysiological overactivation of the MR leads to inflammation and fibrosis in cardiorenal disease. We discuss the mechanisms of action of nonsteroidal MRAs and how they differ from steroidal MRAs. Nonsteroidal MRAs have demonstrated important differences in their distribution, binding mode to the MR and subsequent gene expression. For example, the novel nonsteroidal MRA finerenone has a balanced distribution between the heart and kidney compared with spironolactone, which is preferentially concentrated in the kidneys. Compared with eplerenone, equinatriuretic doses of finerenone show more potent anti-inflammatory and anti-fibrotic effects on the kidney in rodent models. Overall, nonsteroidal MRAs appear to demonstrate a better benefit–risk ratio than steroidal MRAs, where risk is measured as the propensity for hyperkalaemia. Among patients with Type 2 diabetes, several Phase II studies of finerenone show promising results, supporting benefits on the heart and kidneys. Furthermore, finerenone significantly reduced the combined primary endpoint (chronic kidney disease progression, kidney failure, or kidney death) vs. placebo when added to the standard of care in a large Phase III trial.
Introduction
This review aims to provide an overview of the role of the mineralocorticoid receptor (MR) in inflammation and fibrosis and to discuss the discovery of agents that target the MR. We first explore steroidal MR antagonists (MRAs), such as spironolactone and eplerenone, and then the nonsteroidal MRAs. We also endeavour to conceptualize the molecular mechanisms of MR antagonism and downstream cardiorenal protection to better distinguish how the mechanisms of action of nonsteroidal MRAs differ from those of steroidal MRAs. Preclinical studies are described to set the stage for presenting nonsteroidal MRAs as a new treatment option in patients with cardiorenal disease. Specifically, in patients with Type 2 diabetes (T2D) and cardiorenal disease, we discuss why inflammation and fibrosis mediated by MR overactivation could present a novel treatment target beyond traditional treatments focusing primarily on metabolic and haemodynamic targets. Finerenone and esaxerenone are two new nonsteroidal MRAs under clinical development to treat patients with chronic kidney disease (CKD) and T2D.1–3
Steroid hormone receptors and their ligands
Steroid hormone receptors comprise a subfamily of nuclear receptors that act as intracellular receptors and nuclear transcription factors. This subfamily consists of the androgen receptor, the glucocorticoid receptor (GR), the MR, the progesterone receptor, and oestrogen receptors. The GR is activated by cortisol, whereas the MR is promiscuous with the same binding affinity for aldosterone and cortisol.4 MRs mediate fluid, electrolyte, and haemodynamic homeostasis, as well as tissue repair.4 GR modulation impacts energy homeostasis, stress responses, and inflammation.4 Because MRs and GRs are often expressed in the same tissues and cells, regulating their functional interactions is key to maintaining homeostatic balance.4 Interestingly, progesterone also acts as an endogenous MRA because it can compete with aldosterone for MR binding with similar affinity.4
Discovery of the pro-inflammatory and pro-fibrotic effects of aldosterone and the development of spironolactone
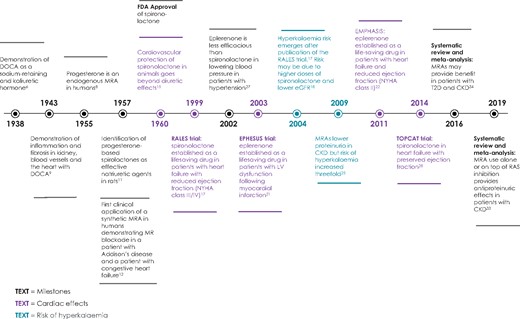
The purification of deoxycorticosterone acetate (DOCA)5 facilitated experiments to gain insights into its physiology and pharmacology as a potent MR agonist. In 1938, Thorn et al. 6 demonstrated that dogs treated with DOCA had sodium chloride retention and potassium diuresis (Figure 1). In the same year, Thorn and Engel7 noted progesterone as a potential adrenal replacement therapy, but these experiments were marred by the large supplies of progesterone needed. Progesterone was not recognized as an MRA until 1955; this finding provided an explanation for the escape from aldosterone-induced sodium retention during pregnancy.8
Key studies in the history of mineralocorticoid receptor antagonists.
In 1943, Selye et al.9 performed seminal experiments noting the central importance of MR agonists on target organ damage. A 2 × 2 factorial trial of salt and DOCA was performed in rats (aldosterone was unavailable at the time). Malignant hypertension, produced by DOCA and salt in combination, was associated with inflammation and fibrosis in various organs (i.e. malignant nephrosclerosis, cardiac hypertrophy, rigid aorta, and oedematous pancreatitis).9 While increased blood pressure (BP) and salt were necessary, it was inflammation and fibrosis that caused organ damage. These historical findings have been replicated with aldosterone in models demonstrating reactive and progressive interstitial and perivascular fibrosis, such as perivascular coronary fibrosis in rats.10
In 1957, two separate papers provided early examples of bench-to-bedside and academia–industry collaboration.11 , 12 The first was a preclinical study showing aldosterone antagonism by new steroidal drugs SC-5233 and SC-8109 (modified from progesterone with relative activities 7.5 and 26.8, respectively).11 The second was a clinical paper by Liddle12 demonstrating that SC-5233 caused potassium retention and sodium secretion both in a patient with congestive heart failure (HF) and in DOCA-treated patients with Addison’s disease.
SC-5233 and SC-8109 use was limited by the need for subcutaneous administration. This barrier was surmounted in 1957 by the synthesis of an active steroidal MRA, spironolactone, that could be administered orally. This important discovery facilitated implementation in clinical trials,13 and within 3 years of its synthesis, the US Food and Drug Administration approved spironolactone, which had a 46-fold more potent oral activity than SC-5233. Spironolactone was launched as a diuretic for the management of oedematous conditions, primary aldosteronism, and essential hypertension.14
Following the discovery and availability of spironolactone, Selye demonstrated attenuation of aldosterone effects and salt on cardiac necrosis using spironolactone in animals. In the presence of a high-salt diet, spironolactone provided a 40% risk reduction in cardiac necrosis but demonstrated complete protection (100% risk reduction) in the absence of salt; this animal model shows that both a low-salt diet and spironolactone are required to observe the full treatment benefits of MR antagonism.15 The pharmacology and science of MRAs is beyond the scope of this work but is reviewed elsewhere.16
Resurrection of steroidal mineralocorticoid receptor antagonists
Summary of key clinical trials in cardiac diseases
Despite preclinical data on BP lowering and cardiorenal protection, it was not until 1999 that the first seminal trial with spironolactone in patients with HF with reduced ejection fraction (HFrEF) was published.17 Results of the Randomized Aldactone Evaluation Study (RALES; N = 1663) showed that spironolactone (∼25 mg/day) reduced the risk of death by 30% vs. placebo [hazard ratio (HR) = 0.70; 95% confidence interval (CI) 0.60–0.82; P < 0.001) in patients with HFrEF New York Heart Association (NYHA) Class III–IV [left ventricular ejection fraction (LVEF) <35%).17 The effects were so robust that the trial was stopped prematurely for efficacy. Incidences of progressive HF and sudden death were reduced; HR for hospitalization for heart failure (HHF) was 0.65; and NYHA class improved. However, rates of breast pain and gynaecomastia increased (10% with spironolactone vs. 1% with placebo).17
The major limitation of aldosterone blockade with spironolactone was hyperkalaemia. In 2004, a pharmacoepidemiological study noted an increased incidence of hyperkalaemia after the RALES publication; this also correlated with an increase in prescription of spironolactone.17 The increased incidence of hyperkalaemia was likely related to spironolactone use in patients who would have been excluded from RALES [i.e. those with low estimated glomerular filtration rate eGFR)], and to the use of higher spironolactone doses than that used in RALES.18 A more judicious use of spironolactone and closer patient monitoring may reduce the occurrence of hyperkalaemia.19 , 20
Eplerenone was subsequently developed as a more selective version of spironolactone, with another seminal trial to test its effects among myocardial infarction (MI) patients with an LVEF ≤40% and symptomatic HF.21 Results of the Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study (EPHESUS; N = 6642) showed that eplerenone was associated with a 15% relative risk reduction in all-cause mortality compared with placebo and a 13% relative risk reduction in cardiovascular (CV) mortality or hospitalization due to CV causes compared with placebo.21
In 2011, the Eplerenone in Mild Patients Hospitalization and Survival Study in Heart Failure (EMPHASIS-HF; N = 2737) showed that compared with placebo, eplerenone substantially reduced the risk of death and both the risk of all-cause hospitalization and HHF among patients with LVEF ≤30% and a recent (≤6 months) admission for CV reasons and mild HF symptoms (NYHA Class II).22 Eplerenone has also been studied in patients with acute coronary syndrome without HF in the Impact of Eplerenone on Cardiovascular Outcomes in Patients Post Myocardial Infarction (REMINDER; N = 1012) trial.23 Treatment with eplerenone was found to be safe and well tolerated, but early MRA use did not demonstrate any clear benefit in patients admitted for MI when added to standard of care (SOC). Although the hyperkalaemia rate was higher with eplerenone vs. placebo, no sexual adverse events were reported, unlike those observed for spironolactone in RALES. Despite the demonstrated efficacy and safety of eplerenone, its use in routine clinical practice in patients with CKD is limited.24 This may be due to the associated hyperkalaemia risk,24 , 25 in addition to contraindications in the label for its use in patients with hypertension and concomitant T2D with microalbuminuria.26
Important drug disposition differences were recognized between spironolactone and eplerenone and translated into clinical benefits and harms. In a small head-to-head study of patients with mild-to-moderate hypertension, eplerenone was well tolerated with an adverse event incident rate similar to that of placebo;27 increases in serum aldosterone, total/active plasma renin, and serum potassium were significantly smaller with eplerenone, which paralleled the relatively reduced BP-lowering efficacy of eplerenone (25–50% less potent) compared with spironolactone; no incidence of impotence, gynaecomastia, or dysmenorrhoea was reported with eplerenone.27
In 2014, the Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist (TOPCAT; N = 3445) trial demonstrated that spironolactone (15–45 mg/day) did not reduce the risk for the primary outcome (a composite of CV death, aborted cardiac arrest, or HHF), in patients with symptomatic HF with preserved ejection fraction (LVEF ≥45%) vs. placebo (HR = 0.89; 95% CI 0.77–1.04; P = 0.14).28 In a post hoc subgroup analysis of the trial, spironolactone was associated with a significant reduction in the primary outcome for patients in the Americas but not in Eastern Europe.29 Spironolactone treatment was associated with increased serum creatinine levels and a doubling of the rate of hyperkalaemia (potassium ≥5.5 mmol/L).28
In 2016, the Aldosterone Blockade Early After Acute Myocardial Infarction (ALBATROSS; N = 1603) trial was published.30 Patients with acute MI were randomized to receive an MRA regimen with a single intravenous bolus of potassium canrenoate (200 mg) followed by oral spironolactone (25 mg once daily) for 6 months plus SOC or SOC alone. The primary outcome (a composite of death, resuscitated cardiac arrest, significant ventricular arrhythmia, indication for implantable defibrillator, or new or worsening HF at 6 months) occurred in 11.8% and 12.2% of patients in the treatment and control groups, respectively (HR = 0.97; 95% CI 0.73–1.28), demonstrating no benefit of early MRA use when added to SOC in patients admitted for MI. Hyperkalaemia (potassium ≥5.5 mmol/L) occurred in 3% and 0.2% of patients in the treatment and SOC groups, respectively (P < 0.0001).
Summary of key clinical trials in chronic kidney disease
Despite growing evidence for MRA use in HF, data from clinical trials of MRAs were sparse in patients with kidney failure. To address this, a proof-of-concept study assessed whether steroidal MRAs could protect the heart of patients with CKD Stages II and III receiving an angiotensin-converting enzyme inhibitor (ACEi) or angiotensin receptor blocker (ARB) (N = 112).31 Spironolactone treatment resulted in reduced left ventricular mass and improved arterial stiffness after 40 weeks that was BP independent.31
In 2014, a Cochrane Database Systematic Review extended these observations to 27 studies (N = 1549) but covered fewer patients than those in RALES alone.17 , 32 Hard endpoints such as end-stage kidney disease (ESKD) or major adverse CV effects were not noted in these trials. Spironolactone decreased proteinuria and BP; however, aldosterone antagonist treatment had imprecise effects at the end of treatment on glomerular filtration rate (GFR) (nine studies, N = 528; mean difference −2.55 mL/min/1.73 m2, 95% CI −5.67 to 0.51). Steroidal MRAs doubled the risk of hyperkalaemia (11 studies, N = 632) with a risk ratio (RR) of 2.00 (95% CI 1.25–3.20), and a number needed to treat for an additional harmful outcome (NNTH) of 7.2 (95% CI 3.4 to ∞). Spironolactone increased the risk of gynaecomastia compared with ACEis or ARB or both (four studies, N = 281): RR = 5.14, 95% CI 1.14–23.23; NNTH = 14.1, 95% CI 8.7–37.3.32 An updated 2019 systematic review evaluated the role of MRAs alone or on top of ACEi/ARB (31 studies, N = 2767) and noted that MRA addition was associated with a change in eGFR of −2.38 mL/min/1.73 m2 (95% CI −3.51 to −1.25).33
A 2016 meta-analysis limited observations to patients on dialysis (nine trials, N = 829). MRAs reduced CV mortality in patients receiving dialysis by 66% but increased hyperkalaemia risk threefold vs. controls.34 Following this meta-analysis, the multicentre feasibility study, Safety and CV efficacy of spironolactone in dialysis-dependent ESRD (SPin-D), did not demonstrate CV benefit for spironolactone; rate of hyperkalaemia (potassium >6.5 mmol/L) was similar between placebo and spironolactone 25 mg but increased with spironolactone 50 mg.35
Steroidal MRAs have a relative or absolute contraindication in late-stage CKD. Efforts to find a signal for the efficacy and safety of spironolactone (25 mg) are ongoing in two Phase III placebo-controlled trials in patients receiving dialysis. The Aldosterone bloCkade for Health Improvement EValuation in End-stage renal disease (ACHIEVE) trial will assess CV death or HHF events as the primary outcome in patients with T2D.36 The ALdosterone antagonist Chronic HEModialysis Interventional Survival Trial (ALCHEMIST) will assess time to first incident of non-fatal MI, acute coronary syndrome, HHF, non-fatal stroke, or CV death as the primary outcome in patients with or without T2D.36
Summary of the development of steroidal mineralocorticoid receptor antagonists
The remarkable progress in the development of MRAs is summarized in Figure 1. Up to the 1970s, DOCA synthesis contributed to research on the physiology, pharmacology, and pathophysiology of MR agonists; progesterone was identified as a natural MRA; and parenteral and oral drugs were developed as MRA (outlined in the next section). This was followed by a ∼30-year hiatus, after which lifesaving benefits of MRAs for patients with HFrEF17 culminated in a Level 1A recommendation in clinical guidelines.37 A critical unmet need exists to slow progression of CKD to ESKD, especially in patients with T2D. In CKD, use of steroidal MRAs in preclinical studies demonstrates benefit, but the associated side effects, including hyperkalaemia, persist as the main limitations for broad implementation in clinical use for CV and kidney protection.
Molecular mechanisms of mineralocorticoid receptor antagonism and cardiorenal protection: lessons from animal models
Following cloning of the MR gene in 1987,38 a series of recombinant MR animal models provided molecular insights into the mechanism of action of this receptor (Supplementary material online, Table S1). Collectively, these studies demonstrate that, although the MR is essential for normal kidney and cardiac function,39 overactivation leads to increased reactive oxygen species, inflammation and fibrosis, and ultimately, kidney and CV disease.
In utero complete MR knock-out (MRKO) was lethal within 10 days of birth, eliciting a phenotype of severe pseudohypoaldosteronism in mice, underscoring the critical importance of the MR in salt, water, and BP maintenance during development.40 As expected, an elevated concentration of renin and aldosterone, and decreased epithelial sodium channel (ENaC)-mediated Na+ transport was observed in the colon and kidneys.40 The latter occurred without a reduction in the mRNA abundance of ENaC, suggesting post-transcriptional effects.40 In contrast, MRKO limited to the principal cells of renal tubules permits survival to adulthood; however, abundant dietary sodium is required to compensate for reduced ENaC trafficking.41–43 In contrast, MR overexpression results in abnormalities such as renal enlargement and cardiomyopathy and can be lethal in utero or the early postnatal period.44 , 45
Cardiomyocyte MRKO has been evaluated in various forms of cardiac disease. In an MI mouse model, compared with wild-type controls, MRKO resulted in a number of salutary effects including increased infarct healing, increased myocardial capillary density, decreased pulmonary oedema, improved cardiac remodelling, and reduced contractile dysfunction.46 Cardiomyocyte MRKO prevented MI-associated up-regulation of Nox2 and superoxide production; reduced extracellular matrix deposition; and increased stress-induced activation and subsequent suppression of nuclear factor-κB and decreased apoptosis.46 Reduced inflammation and fibrosis was also demonstrated with cardiomyocyte MRKO in a DOCA–salt-induced mouse model of cardiac fibrosis; these effects were BP independent.47 The cardiomyocyte MRKO model elegantly demonstrates the dissociation between haemodynamic and pro-inflammatory/pro-fibrotic effects of MR activation.
Myeloid MRKO has perhaps contributed the most intriguing results to understanding the molecular physiology and pathophysiology of the MR, suggesting a novel immune mediation of inflammatory and fibrotic processes leading to organ dysfunction. Surprisingly, in a mouse model of glomerulonephritis, podocyte MRKO provided no kidney protection vs. wild-type controls; cystatin C (a marker of kidney function) and histology were similar between groups.48 Contrastingly, myeloid MRKO was renoprotective, with reduced proteinuria vs. wild-type controls.48 Importantly, whereas eplerenone-treated wild-type mice also had reduced proteinuria, unlike myeloid MRKO, eplerenone use was associated with impairment in kaliuresis.48 This is particularly relevant in providing direct evidence of kidney protection by tissue/cell type-selective MR antagonism, without hyperkalaemia.48 Myeloid MRKO has also been shown to be protective against cardiac hypertrophy, fibrosis, and vascular damage. This is intriguing because myeloid MRKO induced a BP increase relative to wild-type mice, not a reduction.49 Furthermore, an ischaemic reperfusion model in myeloid MRKO demonstrated a 65% reduction in infarct volume vs. controls.50 An important role for the MR in inflammation and fibrosis in cardiac disease was identified in this model—compared to wild-type controls, myeloid MRKO mice exhibit a transcription profile of alternative activation in macrophages,49 decreased recruitment of macrophages, suppression of M1 macrophages, and partial restoration of M2 macrophages.41 , 50 Further research showed that activation of the c-Jun NH2-terminal kinase pathway in macrophages after tissue injury is implicated in downstream inflammation and fibrosis.51
The glucocorticoid-inactivating enzyme 11 beta-hydroxysteroid dehydrogenase 2 (11βHSD2) inactivates cortisol in the kidneys, colon, and sweat glands, and its blockade results in activation of the MR by cortisol due to its equal affinity but higher abundance relative to aldosterone.52 Differential MR effects between the heart and kidneys may be mediated by differential 11βHSD2 tissue expression.52 , 53 For example, 11βHSD2 is present in the distal nephron epithelium, where aldosterone activates the MR to stimulate sodium and potassium transport53 but is absent in cardiomyocytes, podocytes, and macrophages,53 suggesting cortisol as the major active MR ligand in these cells. Increased plasma aldosterone has been reported with long-term ACEi/ARB use in patients with congestive HF, CKD, or hypertension, because of incomplete suppression of serum aldosterone levels (aldosterone breakthrough), which may contribute to MR overactivation.54
Steroidal and nonsteroidal antagonism in the steroid hormone receptor family
Following ligand binding, steroid hormone receptors interact with cofactors, including transcriptional cofactors that affect gene transcription. Over 300 different cofactors interact with members of the nuclear hormone superfamily in a ligand- and cell type-specific way, resulting in different physiological responses.55 These differences translate into clinically meaningful differences between steroidal and nonsteroidal ligands. Even within the class of non-steroidal antagonists, remarkably different effects on the androgen receptors have been observed, for example the nonsteroidal anti-androgen drugs enzalutamide and bicalutamide; in recent trials, these molecular pathways translate to meaningful differences in important patient outcomes.56 , 57
Nonsteroidal mineralocorticoid receptor antagonism for cardiorenal disease
Results of RALES17 and EPHESUS21 trials, and a subsequent observation of high incidence of spironolactone-associated hyperkalaemia in clinical practice,58 sparked considerable efforts to identify potent, yet selective, nonsteroidal MRAs for cardiorenal medicine with a favourable benefit–risk profile. Technological advances, such as cloning human MR complementary DNA38 and high-throughput screening assays, led to the discovery of novel, nonsteroidal MRAs.59 Several pharmaceutical companies are investigating this new class of compounds, some of which include: LY 2623091 (Eli Lilly; no longer in development), PF-03882845 (Pfizer; no longer in development), AZD9977 (AstraZeneca; Phase I), apararenone (Mitsubishi Tanabe; unknown status after Phase II), KBP-5074 (KBP Biosciences; Phase II), esaxerenone (Daiichi Sankyo; launched in Japan for hypertension), and finerenone (Bayer AG; Phase III).16 , 60
Several key differences exist between steroidal and nonsteroidal MRAs. Most of the available evidence exploring these differences is available for finerenone; therefore, in this section and in Table 1, we have focused our discussion on the characteristics of steroidal MRAs with those of finerenone. Finerenone is a novel, selective, nonsteroidal MRA, currently under investigation in patients with CKD and T2D to slow the progression of kidney disease and reduce risk of CV events.1 , 2 We draw from other nonsteroidal MRAs where relevant comparisons are available.69–71 Other nonsteroidal MRAs have different physicochemical and pharmacological properties, but corresponding comparisons within this class are pending due to missing data.
Key differences between steroidal MRAs and nonsteroidal finerenone
| Steroidal MRAs | Nonsteroidal finerenone | ||
|---|---|---|---|
| Mode of MR antagonism | Spironolactone | Eplerenone | Finerenone Potent and selective59 Bulky and passive61 |
| Potent and unselective (first generation) | Less potent and more selective than spironolactone (second generation) | ||
| Passive | |||
| Tissue distribution (in rodents) | Spironolactone | Eplerenone | Finerenone: balanced kidney–heart62 |
| Kidney > heart63 | Kidney > heart64 | ||
| Pharmacokinetics | Spironolactone: prodrug with multiple active metabolites with long half-lives65 Eplerenone: no active metabolites; half-life 4–6 h64 | Finerenone: no active metabolites and short half-life66 , 67 | |
| Effect on cofactor recruitment in absence of aldosterone in vitro 61 , 68 | Spironolactone and eplerenone: partial agonistic cofactor recruitment | Finerenone: inverse agonist (inhibits cofactor binding in the absence of aldosterone) | |
| Effect on cofactor recruitment in the presence of aldosterone in vitro | Spironolactone and eplerenone: inhibition of cofactor recruitment68 | Finerenone: more potent and efficacious than eplerenone in blocking MR cofactor binding and inducing corepressor binding68 | |
| Effect on mutated (S810L) MR in vitro 61 | Spironolactone and eplerenone: agonists | Finerenone: antagonist | |
| Effect on inflammation and fibrosis in mouse model of cardiac fibrosis68 | Eplerenone (at equinatriuretic dose to finerenone): less significant effects on inflammation and fibrosis | Finerenone (at equinatriuretic dose to eplerenone): strong inhibition of inflammation and fibrosis | |
| Effect on renal inflammation and fibrosis in a DOCA–salt rat model of CKD62 | Eplerenone (at equinatriuretic dose to finerenone): significant BP reduction; less efficacious proteinuria and renal injury reduction | Finerenone (at equinatriuretic dose to eplerenone): significant systolic BP reduction only at highest dosage; greater protection from cardiac and renal injury and structural remodelling; stronger inhibition of renal expression of pro-inflammatory and pro-fibrotic markers | |
| Steroidal MRAs | Nonsteroidal finerenone | ||
|---|---|---|---|
| Mode of MR antagonism | Spironolactone | Eplerenone | Finerenone Potent and selective59 Bulky and passive61 |
| Potent and unselective (first generation) | Less potent and more selective than spironolactone (second generation) | ||
| Passive | |||
| Tissue distribution (in rodents) | Spironolactone | Eplerenone | Finerenone: balanced kidney–heart62 |
| Kidney > heart63 | Kidney > heart64 | ||
| Pharmacokinetics | Spironolactone: prodrug with multiple active metabolites with long half-lives65 Eplerenone: no active metabolites; half-life 4–6 h64 | Finerenone: no active metabolites and short half-life66 , 67 | |
| Effect on cofactor recruitment in absence of aldosterone in vitro 61 , 68 | Spironolactone and eplerenone: partial agonistic cofactor recruitment | Finerenone: inverse agonist (inhibits cofactor binding in the absence of aldosterone) | |
| Effect on cofactor recruitment in the presence of aldosterone in vitro | Spironolactone and eplerenone: inhibition of cofactor recruitment68 | Finerenone: more potent and efficacious than eplerenone in blocking MR cofactor binding and inducing corepressor binding68 | |
| Effect on mutated (S810L) MR in vitro 61 | Spironolactone and eplerenone: agonists | Finerenone: antagonist | |
| Effect on inflammation and fibrosis in mouse model of cardiac fibrosis68 | Eplerenone (at equinatriuretic dose to finerenone): less significant effects on inflammation and fibrosis | Finerenone (at equinatriuretic dose to eplerenone): strong inhibition of inflammation and fibrosis | |
| Effect on renal inflammation and fibrosis in a DOCA–salt rat model of CKD62 | Eplerenone (at equinatriuretic dose to finerenone): significant BP reduction; less efficacious proteinuria and renal injury reduction | Finerenone (at equinatriuretic dose to eplerenone): significant systolic BP reduction only at highest dosage; greater protection from cardiac and renal injury and structural remodelling; stronger inhibition of renal expression of pro-inflammatory and pro-fibrotic markers | |
BP, blood pressure; CKD, chronic kidney disease; DOCA, deoxycorticosterone acetate; MR, mineralocorticoid receptor; MRA, mineralocorticoid receptor antagonist.
Key differences between steroidal MRAs and nonsteroidal finerenone
| Steroidal MRAs | Nonsteroidal finerenone | ||
|---|---|---|---|
| Mode of MR antagonism | Spironolactone | Eplerenone | Finerenone Potent and selective59 Bulky and passive61 |
| Potent and unselective (first generation) | Less potent and more selective than spironolactone (second generation) | ||
| Passive | |||
| Tissue distribution (in rodents) | Spironolactone | Eplerenone | Finerenone: balanced kidney–heart62 |
| Kidney > heart63 | Kidney > heart64 | ||
| Pharmacokinetics | Spironolactone: prodrug with multiple active metabolites with long half-lives65 Eplerenone: no active metabolites; half-life 4–6 h64 | Finerenone: no active metabolites and short half-life66 , 67 | |
| Effect on cofactor recruitment in absence of aldosterone in vitro 61 , 68 | Spironolactone and eplerenone: partial agonistic cofactor recruitment | Finerenone: inverse agonist (inhibits cofactor binding in the absence of aldosterone) | |
| Effect on cofactor recruitment in the presence of aldosterone in vitro | Spironolactone and eplerenone: inhibition of cofactor recruitment68 | Finerenone: more potent and efficacious than eplerenone in blocking MR cofactor binding and inducing corepressor binding68 | |
| Effect on mutated (S810L) MR in vitro 61 | Spironolactone and eplerenone: agonists | Finerenone: antagonist | |
| Effect on inflammation and fibrosis in mouse model of cardiac fibrosis68 | Eplerenone (at equinatriuretic dose to finerenone): less significant effects on inflammation and fibrosis | Finerenone (at equinatriuretic dose to eplerenone): strong inhibition of inflammation and fibrosis | |
| Effect on renal inflammation and fibrosis in a DOCA–salt rat model of CKD62 | Eplerenone (at equinatriuretic dose to finerenone): significant BP reduction; less efficacious proteinuria and renal injury reduction | Finerenone (at equinatriuretic dose to eplerenone): significant systolic BP reduction only at highest dosage; greater protection from cardiac and renal injury and structural remodelling; stronger inhibition of renal expression of pro-inflammatory and pro-fibrotic markers | |
| Steroidal MRAs | Nonsteroidal finerenone | ||
|---|---|---|---|
| Mode of MR antagonism | Spironolactone | Eplerenone | Finerenone Potent and selective59 Bulky and passive61 |
| Potent and unselective (first generation) | Less potent and more selective than spironolactone (second generation) | ||
| Passive | |||
| Tissue distribution (in rodents) | Spironolactone | Eplerenone | Finerenone: balanced kidney–heart62 |
| Kidney > heart63 | Kidney > heart64 | ||
| Pharmacokinetics | Spironolactone: prodrug with multiple active metabolites with long half-lives65 Eplerenone: no active metabolites; half-life 4–6 h64 | Finerenone: no active metabolites and short half-life66 , 67 | |
| Effect on cofactor recruitment in absence of aldosterone in vitro 61 , 68 | Spironolactone and eplerenone: partial agonistic cofactor recruitment | Finerenone: inverse agonist (inhibits cofactor binding in the absence of aldosterone) | |
| Effect on cofactor recruitment in the presence of aldosterone in vitro | Spironolactone and eplerenone: inhibition of cofactor recruitment68 | Finerenone: more potent and efficacious than eplerenone in blocking MR cofactor binding and inducing corepressor binding68 | |
| Effect on mutated (S810L) MR in vitro 61 | Spironolactone and eplerenone: agonists | Finerenone: antagonist | |
| Effect on inflammation and fibrosis in mouse model of cardiac fibrosis68 | Eplerenone (at equinatriuretic dose to finerenone): less significant effects on inflammation and fibrosis | Finerenone (at equinatriuretic dose to eplerenone): strong inhibition of inflammation and fibrosis | |
| Effect on renal inflammation and fibrosis in a DOCA–salt rat model of CKD62 | Eplerenone (at equinatriuretic dose to finerenone): significant BP reduction; less efficacious proteinuria and renal injury reduction | Finerenone (at equinatriuretic dose to eplerenone): significant systolic BP reduction only at highest dosage; greater protection from cardiac and renal injury and structural remodelling; stronger inhibition of renal expression of pro-inflammatory and pro-fibrotic markers | |
BP, blood pressure; CKD, chronic kidney disease; DOCA, deoxycorticosterone acetate; MR, mineralocorticoid receptor; MRA, mineralocorticoid receptor antagonist.
Comparison between nonsteroidal mineralocorticoid receptor antagonist (finerenone) and steroidal mineralocorticoid receptor antagonists
Mode of mineralocorticoid receptor antagonism
Nuclear receptors such as the MR comprise discrete domains for specific functions including ligand binding, activation, and DNA recognition. There are at least 22 known cofactors that associate with MR72 that determine the full transcriptional response mediated by the MR in a cell-specific manner.68 , 72 Molecular modelling studies of the finerenone–MR complex suggest that finerenone blocks the MR as a bulky, passive antagonist. This mechanism is distinct from steroidal MRAs, which might impact its differential clinical response.61 Finerenone’s unique binding mode determines potency, selectivity, and nuclear cofactor recruitment, while its physicochemical properties, including lipophilicity and polarity, determine tissue penetration and distribution, which in combination offer a novel MRA pharmacology with pronounced anti-fibrotic efficacy in animal models. Compared with other MRAs, finerenone has differential downstream effects on MR blockade (Figure 2). Finerenone is more selective for the MR than eplerenone and spironolactone and is at least as potent as spironolactone.16
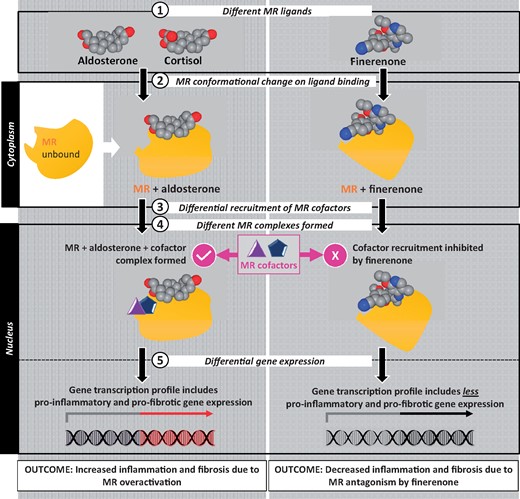
Finerenone reduces cofactor recruitment to the mineralocorticoid receptor, thereby reducing downstream expression of pro-inflammatory and pro-fibrotic factors following mineralocorticoid receptor overactivation. MR, mineralocorticoid receptor.
Tissue distribution
Experiments using [14C]-labelled eplerenone or [3H]-spironolactone demonstrated a higher accumulation of drug-equivalent concentrations in kidney vs. heart tissue in rodents, whereas [14C]-labelled finerenone demonstrated a balanced kidneys–heart distribution in rats.62–64 This may contribute to the greater effect of spironolactone and eplerenone on sodium and potassium balance.62 In addition, finerenone does not cross the blood–brain barrier; finerenone was not detected in brain tissue following oral application of the radio-labelled drug in preclinical studies.73
Pharmacokinetics
Differential effects have been observed with once-daily and twice-daily dosing of MRAs, suggesting that length of exposure might influence pharmacodynamic response.16 For example, eplerenone twice daily (half-life of 4–6 h)64 has a greater BP-lowering effect than once-daily administration;27 however, single daily dosing is sufficient to observe mortality benefits in HF.21 It is, therefore, hypothesized that effects including BP control and serum potassium changes may result from longer MRA exposure and that the anti-inflammatory and anti-fibrotic response might be exerted via a signalling cascade that can be sufficiently blocked by a shorter MRA exposure.16 Compared with steroidal MRAs, finerenone has greater polarity and is 6- to 10-fold less lipophilic.60 Kidney elimination of finerenone is minimal; it has a short half-life (2–3 h in patients with kidney failure) and no active metabolites.66 , 67 , 74 Conversely, spironolactone is a prodrug with biologically active metabolites (e.g. canrenone and 7-α-thiomethylspironolactone), which have long half-lives and can accumulate over time.65 This is evident in a clinical setting, where spironolactone metabolites were measured in patients with eGFR 25–45 mL/min/1.73 m2: 38% of patients had detectable urinary levels of metabolites up to 3 weeks after stopping treatment (Figure 3). In fact, over half of the systolic BP-lowering effect was retained 2 weeks after stopping treatment, suggesting that the metabolite-induced haemodynamic effects had persisted especially among patients with moderate-to-advanced CKD.75 Likely, spontaneous recovery from hyperkalaemia may not be expected immediately after spironolactone discontinuation.
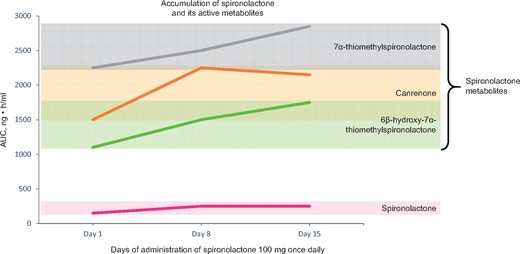
Mean relative exposure of spironolactone and spironolactone metabolites in healthy volunteers (n = 12). AUC, area under the concentration–time curve.
Effect on cofactor recruitment to the mineralocorticoid receptor complex in the presence or absence of aldosterone
Finerenone can act in vitro as an inverse agonist to the MR, i.e. reducing cofactor recruitment even in the absence of aldosterone, whereas spironolactone and eplerenone exhibit partial agonism on cofactor recruitment, but to a lesser extent than aldosterone.61 , 68 This suggests that, unlike other MRAs, finerenone blocks deleterious gene activation by the MR independently of aldosterone.60 , 68 Finerenone also blocks the human mutant MR, S810L, which is activated by both progesterone and steroidal MRAs (spironolactone and eplerenone) and associated with hypertension during pregnancy.61 , 76 The combination of a specific antagonistic binding mode for finerenone with its physicochemical properties yielded in a novel MRA pharmacology with a pronounced anti-hypertrophic/-fibrotic efficacy for a given natriuretic activity, as demonstrated in preclinical models.16 , 60 , 68
Electrolyte effects vs. anti-fibrotic effects
Both eplerenone77 and finerenone78 have been associated with anti-fibrotic effects in preclinical studies. MR antagonism decreases macrophage expression of the pro-fibrotic genes tumour growth factor-β1 and plasminogen activator inhibitor-1 and increases the expression of anti-fibrotic genes.79
In models of kidney injury, finerenone reduced the expression of pro-inflammatory and pro-fibrotic markers and reduced proteinuria and tubulointerstitial fibrosis, including at doses that did not significantly affect BP.62 , 80 Compared with eplerenone at equinatriuretic doses, finerenone was associated with less kidney hypertrophy, proteinuria, and renal pro-inflammatory/pro-fibrotic gene expression in response to kidney injury.62 Compared with eplerenone in models of cardiac fibrosis, finerenone also demonstrated qualitatively different effects on pro-fibrotic gene expression and measures of inflammation and fibrosis.62 , 68 However, the benefits of MRAs on kidney and cardiac outcomes need to be balanced against the risk of hyperkalaemia. A nonsteroidal MRA (PF-03882845) was compared with eplerenone in a rat model of CKD81 and a therapeutic index was calculated as the ratio of drug concentration that increased serum potassium to the respective drug concentration that lowered urinary albumin. This was 1.5-fold for eplerenone but 84-fold for PF-03882845,81 providing further evidence for a reduced risk of hyperkalaemia with the nonsteroidal MRA PF-03882845 vs. steroidal MRA in a relevant preclinical CKD model.
Clinical development programme of nonsteroidal mineralocorticoid receptor antagonists
Two nonsteroidal MRAs have progressed into Phase III development: finerenone and esaxerenone. The first large Phase III trial on finerenone’s kidney outcomes (FIDELIO-DKD; N = 5734) in patients with CKD and T2D was recently completed, meeting its primary endpoint.1 , 82 Two Phase III studies are ongoing for finerenone to investigate its effect on CV outcomes in patients with CKD and T2D (FIGARO-DKD),2 and to evaluate morbidity and mortality outcomes in patients with symptomatic HF (NYHA Class II–IV and LVEF ≥40%; FINEARTS-HF).83 Esaxerenone is approved for the treatment of essential hypertension in Japan.84 Albuminuria reduction was demonstrated in a Phase III trial of patients with T2D and high albuminuria [urine albumin-to-creatinine ratio (UACR) ≥45 to ≤300 mg/g and eGFR ≥30 mL/min/1.73 m2);3 treatment discontinuation rate due to hyperkalaemia was 3%, 3%, and 10% in patients treated with 1.25, 2.5, and 5 mg esaxerenone, respectively, vs. placebo.3 Differences in clinical effects between nonsteroidal MRAs, such as BP and hyperkalaemia, appear to exist based on indirect comparisons, but definitive conclusions cannot be made without head-to-head studies.16
The Phase II ARTS programme investigating finerenone comprised five Phase II studies in over 2000 patients (Figure 4).73 , 85 , 86 ARTS was designed to test the safety and tolerability of finerenone in patients with HFrEF and mild-to-moderate CKD.73 Mean increases in serum potassium concentration were significantly smaller with all doses of finerenone vs. spironolactone 50 mg daily, and decline in eGFR was reduced with finerenone, leading to fewer patients with hyperkalaemia, kidney failure, or kidney impairment (Figure 4).73 The primary endpoint in ARTS-HF was proportion of patients with >30% decline in NT-proBNP from baseline to day 90.86 Achievement of this endpoint was comparable with eplerenone at all finerenone doses tested (2.5–20.0 mg), but the composite secondary endpoint of all-cause mortality, CV hospitalization, and emergency presentation for HF was nominally improved with finerenone 10–20 mg vs. eplerenone. However, these results must be interpreted with caution as the study was not powered to investigate treatment effects on hard outcomes (Figure 4).86 The primary outcome in ARTS-DN of UACR reduction from baseline to day 90 was found to be dose dependent for finerenone (Figure 4).85 This was statistically significant for the four highest doses of finerenone, with a placebo-corrected UACR reduction of 38% at 20 mg/day.85 Post hoc analysis showed that UACR changes were independent of changes in BP or eGFR, suggesting non-haemodynamic effects.85 There were no differences in the overall incidence of adverse events, including an eGFR reduction of ≥30%, between finerenone and placebo.85 The rate of treatment discontinuation due to hyperkalaemia was low and not dose dependent.85
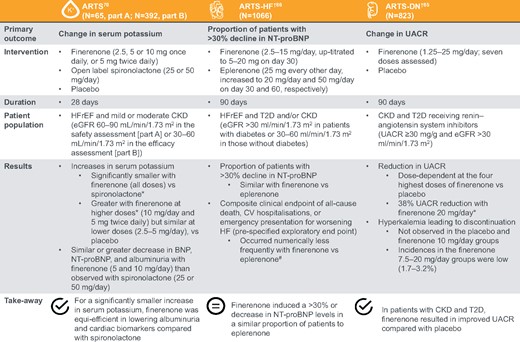
Key results of the ARTS, ARTS-HF, and ARTS-DN Phase II studies. *Significant (P ≤ 0.001); #Nominal statistical significance in the finerenone 10–20 mg group (hazard ratio = 0.56, 95% confidence interval 0.35; 0.90, P = 0.02). CV, cardiovascular; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; HFrEF, heart failure with reduced ejection fraction; NT-proBNP, N-terminal pro-B-type natriuretic peptide; T2D, Type 2 diabetes; UACR, urine albumin-to-creatinine ratio.
A meta-regression analysis of drug trials correlated interventions leading to UACR reductions of 30% with a 23.7% reduced risk of kidney failure (95% CI 11.4–34.2%).87 Based on promising Phase II results from ARTS-DN, with 30–40% UACR reduction at doses with minimal effects on potassium and BP,73 , 85 , 86 finerenone is being investigated in the largest event-driven Phase III clinical programme of CKD in T2D to date; it is powered to detect a 20% relative risk reduction in the primary endpoint. FIDELIO-DKD (NCT02540993) is a randomized, double-blind, placebo-controlled, event-driven study investigating the safety and efficacy of finerenone plus SOC on kidney disease progression in patients with CKD and T2D.1 The primary endpoint was time to first occurrence of onset of kidney failure, a sustained decrease of eGFR ≥40%, or renal death.1 Finerenone significantly reduced the combined primary endpoint and the combined secondary endpoint (time to first occurrence of CV death, non-fatal MI or stroke, or HHF) compared with placebo.82
Conclusions
MR overactivation results in deleterious effects on the kidneys and heart, promoting inflammation and fibrosis, and progression of kidney and CV disease; effects that extend beyond the well-recognized retention of salt and water and downstream hypertension. MRKO studies demonstrated that MR antagonism could play a key role in addressing the residual risk of progression of kidney and heart disease. MRAs can be categorized as steroidal or nonsteroidal, with key differences in molecular and pharmacological properties between them. The novel, nonsteroidal, selective MRA finerenone shows several promising differences from steroidal MRAs in preclinical models, with a mechanism of action distinct from other emerging agents for cardiorenal medicine in CKD and T2D. In the Phase III randomized trial, FIDELIO-DKD, finerenone significantly reduced the primary and secondary composite endpoints vs. placebo, suggesting that finerenone may forestall progression to kidney failure in patients with CKD and T2D.82 The FIGARO-DKD study will further address whether finerenone can reduce the risk of major adverse CV events in this patient population. Combined, these studies should firmly establish the role of finerenone in cardiorenal medicine.
Supplementary material
Supplementary material is available at European Heart Journal online.
Acknowledgements
This study was sponsored by Bayer AG, the manufacturer of finerenone. All authors received travel expenses from Bayer AG to meet and plan the preparation of the manuscript. Medical writing services provided by Savroop Bhamra from Chameleon Communications International were funded by Bayer AG.
Conflict of interest: R.A. reports personal fees from Akebia, during the conduct of the study, personal fees from Bayer, personal fees from Abbvie, personal fees from Astra Zeneca, personal fees from Johnson and Johnson, personal fees from Boehringer Ingelheim, personal fees from Takeda, personal fees from Daiichi Sankyo, personal fees from Amgen, personal fees from Celgene, personal fees from Eli Lilly, personal fees from Relypsa, personal fees from Reata, personal fees from Opko, personal fees from ZS Pharma, and personal fees from Merck, outside the submitted work. G.B. reports other from Bayer, during the conduct of the study, and other from Vascular Dynamics and Novo Nordisk, outside the submitted work. J.B. reports personal fees from Abbott, grants and personal fees from Abiomed, personal fees from Astra Zeneca, personal fees from Bayer, personal fees from BMS, personal fees from Boehringer Ingelheim, grants and personal fees from CvRX, personal fees from Daiichi Sankyo, personal fees from Medtronic, personal fees from MSD, personal fees from Novartis, personal fees from Pfizer, personal fees from Servier, grants and personal fees from Vifor, and grants and personal fees from Zoll, outside the submitted work. H.H. reports personal fees from Bayer AG, during the conduct of the study, personal fees from Alexion Pharma, from AstraZeneca, and from Vifor Pharma, and personal fees from Böhringer AG, outside the submitted work. T.W. reports grants, personal fees, and other from Kyowa Kirin Co., Ltd, grants and personal fees from Mitsubishi Tanabe Pharma Corporation, grants from Chugai Pharmaceutical Co., Ltd, grants from MSD K.K., personal fees from Bayer Yakuhin Ltd, grants and personal fees from Astellas Pharma Inc., personal fees from AstraZeneca K.K., personal fees from Eli Lilly Japan K.K., personal fees from Ono Pharmaceutical Co., Ltd, grants and personal fees from Kissei Pharmaceutical Co., Ltd, personal fees from Kowa Company, Ltd, grants and personal fees from Sanofi K.K., personal fees from Sanwa Chemistry Co., Ltd, grants and personal fees from Daiichi Sankyo Company, Ltd, personal fees from Taisho Pharma Co., Ltd, grants and personal fees from Takeda Pharmaceutical Company Limited, and personal fees from Nippon Boehringer Ingelheim Co., Ltd, outside the submitted work. F.Z. reports personal fees from Bayer, during the conduct of the study, personal fees from Janssen, personal fees from Novartis, personal fees from Boston Scientific, personal fees from Amgen, personal fees from CVRx, personal fees from Boehringer, other from cardiorenal, personal fees from AstraZeneca, personal fees from Vifor Fresenius, personal fees from Cardior, personal fees from Cereno pharmacuetical, personal fees from Applied Therapeutics, personal fees from Merck, and other from CVCT, outside the submitted work. P.K. is a co-inventor of finerenone (patents EP2132206B1 and US8436180B2) and a full-time employee of Bayer AG.
References
Pfizer. Inspra (Eplerenone) US Prescribing Information;
GD Searle LLC. Inspra (Eplerenone) Prescribing Information;
Bayer. Bayer's Finerenone Meets Primary Endpoint in Phase III FIDELIO-DKD Renal Outcomes Study in Patients with Chronic Kidney Disease and Type 2 Diabetes;
Bayer. Study to Evaluate the Efficacy (Effect on Disease) and Safety of Finerenone on Morbidity (Events Indicating Disease Worsening) and Mortality (Death Rate) in Participants with Heart Failure and Left Ventricular Ejection Fraction (Proportion of Blood Expelled per Heart Stroke) Greater or Equal to 40% (FINEARTS-HF);


{kind=link}
{kind=link}
{kind=link}
{kind=link}