





Abstract
Familial hypercholesterolemia (FH) syndromes constitute an important risk factor for premature atherosclerosis. Microwave radiometry (MWR) assess non-invasively carotid artery temperatures reflecting inflammation. Recent data support that statin therapy, that constitutes the cornerstone for the treatment of FH, reduces systemic inflammation.
To investigate the impact of statin therapy either with simvastatin or with combination simvastatin plus ezetimibe on carotid artery temperatures.
Consecutive patients with diagnosis of either heterozygous hypercholesterolemia (hFH) or combined hyperlipidemia (FCH) not under statin therapy for at least 6 months were included in the study. FH pts were assigned to either simvastatin 40 mg or simvastatin 40 mg plus ezetimibe 10mg according to the discretion of the physician. FH patients who refused statin therapy were used as control group for the assessment of statins effect. In all subjects, common carotid intima-media thickness (ccIMT) was measured in the last 2 cm of the far wall of both common carotids close to the carotid bifurcation and ΔT (maximum-minimum) temperature measurements were performed across each carotid during MWR evaluation. Examinations were performed at baseline and after 6 months. Blood's lipid profile was also obtained in all patients.
In total 115 patients were included in the study. Of them 40 patients received simvastatin (19 hFH and 11 FCH), 41 simvastatin + ezetimibe (31hFH and 10 FCH) and 34 (21 hFH and 13 FCH) no statin. There was no difference at baseline in ccIMT and ΔT measurements between hFH and FCH patients (0.10±0.03 vs 0.10±0.02, p=0.74 and 0.88±0.38 vs 0.84±0.32, p=0.52, respectively). Patients who refused statin therapy did not show any reduction in ccIMT and ΔT measurements between baseline and follow up (ccIMT: 0.10±0.02 vs 0.09±0.02, p=0.06 and ΔT: 0.72±0.26 vs 0.70±0.26). In contrast, there was a significant reduction in ccIMT and ΔT for patients under both simvastatin (0.10±0.03 vs 0.09±0.01, p=0.004 for ccIMT and 0.83±0.34 vs 0.63±0.24, p=0.04 for ΔT) and simvastatin + ezetimibe therapy (0.11±0.03 vs 0.09±0.02, p<0.001 and 1.00±0.38 vs 0.69±0.23, p<0.001 for ΔT). Patients under combination therapy reduced more significantly their carotid artery temperatures compared to patients under simvastatin monotherapy or patients without statin (−0.31±0.46 vs −0.2±0.40 vs −0.01±0.37, ANOVA p=0.04, Figure 1).
Both simvastatin and simvastatin + ezetimibe therapy among the beneficial effect on IMT, reduced carotid wall inflammation in FH pts.
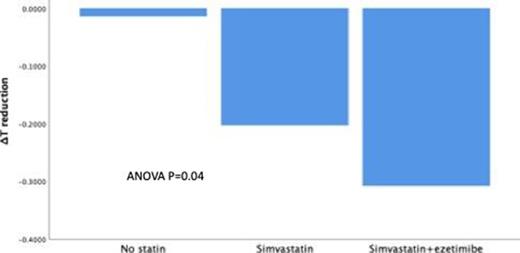
Figure 1
Type of funding source: None


{kind=link}