





Abstract
Recent recommendations by national and international societies advocate the use of coronary computed tomography (CCT) as the first-line test for the assessment of low-risk patients with suspected stable angina. However limited real-life data exist regarding its relative clinical value versus stress echocardiography (SE)-guided management.
We aimed to assess in a real-life setting the clinical value of stress echocardiography (SE)-guided versus CCT-guided management in patients presenting with stable chest pain and no prior history of coronary artery disease (CAD).
We compared the relative feasibility, efficacy and the proportion of patients undergoing downstream testing including revascularisation and their impact on outcome (mortality and myocardial infarction) when CCT versus SE were used as the first line test for the assessment of stable chest pain.
Of the patients who underwent CCT (N=2192) or SE (N=2081) between October 2013 and October 2014 only those with suspected stable angina and without previous CAD were selected. The population was propensity-matched (total 1980 patients-990 patients each group) to account for differences in the baseline cardiovascular risk factors.
The mean age of the population was 59±13.2 years and 949 (47.9%) patients were male. Inconclusive tests were 6% versus 3% (p<0.005) in CCT versus SE. Severe (>70%) luminal stenosis on CCT and inducible ischemia on SE detected obstructive CAD by invasive coronary angiography in 63% versus 57% patients (p=0.33). Over the entire follow-up period (median 717 (IQR 93–1069) days) significantly more patients underwent invasive coronary angiography (21.5% versus 7.3%, p<0.005) and revascularisation (33.5% versus 3.5%, p<0.005) respectively in the CCT versus the SE group. Following their initial assessment 336 (33.9%) patients in the CCT and 86 (8.7%) in the SE group underwent further functional testing (SE, stress cardiac MRI, exercise electrocardiography) (p<0.005) (Figure 1A). There was no difference in all-cause mortality (p=0.26) or death and myocardial infarction (p=0.16) between the two groups (Figure 1B).
SE when used for the assessment of patients with stable angina and no prior CAD resulted in more conclusive tests, similar detection of obstructive CAD, less overall invasive coronary angiography and revascularization and less subsequent functional tests compared with CCT.
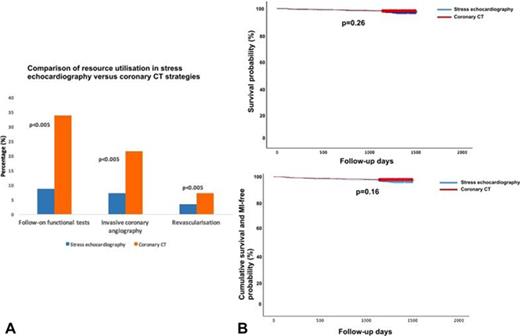
Figure 1
Type of funding source: None


{kind=link}