





Summary
The concept that posterior crossbite is not self-correcting has been controversial in the literature.
To evaluate the incidence of self-correction of crossbite in different stages of dentition in childhood.
A bibliographic search using the acronym PECOS was performed in five databases and in partial grey literature. Studies evaluating children with posterior crossbite in the deciduous or mixed dentition at initial examination and followed for at least 3 years were included.
The data extraction of the studies included presents information on authorship, clinical characteristics, main results, and conclusions. The risk of bias in the studies was evaluated through the Joanna Briggs Institute tool. The certainty of the evidence was assessed using the GRADE tool.
Among the 3045 references identified, seven cohort studies met the eligibility criteria. The studies evaluated patients in transition from deciduous to mixed, mixed to permanent, and deciduous to mixed dentition. Two studies had a low risk of bias, three had a moderate risk, and two had a high risk of bias. The results showed posterior crossbite self-correction frequencies ranging from 12.2 to 77.1% during the transition from primary to mixed dentition, approximately 16% from mixed to permanent dentition, and a range from 20 to 82.8% from deciduous to permanent dentition. The level of certainty of the evidence generated ranged from very low to moderate.
The observational design of the studies, without adequate control for confounding factors, and non-classification of the samples considering the types or the severity of the posterior crossbite.
The self-correction of posterior crossbite in childhood is possible. However, the results of this research do not allow to affirm how often the self-correction of posterior crossbite can occur. New studies that assess factors associated with the occurrence of self-correction of this malocclusion, including oral habits, may increase the certainty of the evidence.
PROSPERO CRD42022311935
Introduction
Posterior crossbite (PCB) is the abnormal transverse relationship, buccal or lingual, of one or more teeth of the upper arch with one or more teeth of the lower arch, and may occur unilaterally or bilaterally (1). This disturbance can be caused by a skeletal transverse discrepancy between the upper and lower dental arches, changes in the buccolingual inclination of the posterior teeth, end-to-end occlusal relationships that generate mandibular deviations in laterality (functional PCB), or even the total involvement of the mandible by the maxilla (2).
It is widely reported in the literature that PCB should be treated early through maxillary expansion (3,4), together with removal of oral habits (5) and occlusal interference (6). Early treatment is indicated based on the premise that this malocclusion can have long-term impacts on dental development and the temporomandibular joint (7). In addition, studies claim that the relatively uniform prevalence in all stages of tooth development suggests that PCB would not have the potential for self-correction (8).
While studies with a relatively short follow-up time (±1 year) reported that untreated PCB did not present self-correction (9,10), studies with longer follow-up times show some frequency of self-correction of PCB in children (11,12).
The concept that PCB is not self-correcting has been controversial and even questionable in the literature. Therefore, the objective of this systematic review was to assess whether there is self-correction of PCB in childhood and analyse in which stages of development this self-correction can occur.
Material and methods
Protocol and registration
This systematic review was registered at PROSPERO database, under registration code CRD42022311935, and prepared following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) (13).
Eligibility criteria
The included studies were selected according to the selection criteria based on the PECOS acronym, where:
P (population): Children in deciduous or mixed dentition at initial assessment followed up for at least three years;
E (exposure): Posterior crossbite;
C (comparison): Before and after of the patient themselves;
O (outcome): Self-correction of posterior crossbite;
S (study design): Controlled and/or randomized clinical studies, and observational studies.
Exclusion criteria consisted of: Children with craniofacial syndromes or anomalies, previous orthodontic treatment, abstracts, case reports, opinion articles and book chapters.
Information sources
The searches were performed according to the PECOS acronym, between March and April 2022, through five electronic databases: PubMed, Scopus, Web of Science, LILACS, and LIVIVO. The grey literature search included OpenGrey and Google Scholar. Also, a manual search was performed in the reference lists of the included articles. No language restrictions were applied, and coverage dates were not limited. Search alerts were verified through 22 May 2023.
Search strategy and selection process
The search strategy was developed for each database with a combination of MeSH/Decs terms and keywords related to the PECOS acronym, associated with the use of the Boolean operators ‘OR’ and ‘AND’ (Supplementary Table 1). A librarian was consulted to design an appropriate search strategy. All relevant citations were exported to a reference management software (EndNote, version x9, Clarivate Analytics, Philadelphia, Pennsylvania, USA).
Two independent reviewers (BN and CS) selected the articles included in two phases. In the first phase, the articles were evaluated by title and abstract according to the eligibility criteria. In phase two, the full texts of potentially relevant studies were evaluated and selected following the same eligibility criteria as in phase one. Then, all the information found was cross-referenced. In case of disagreements during the selection, two other authors (MS and DN) were consulted.
Data collection process and data items
The data extraction of the studies included in the review presents information on authorship (author, year of publication, and study design), clinical characteristics (sample size, sex, and age, follow-up time and evaluated dentitions, PCB classification, presence of oral habits, PCB diagnosis method, statistical analysis performed, and diagnosis of self-correction of posterior crossbite); main results (PCB self-correction and association with oral habits); and conclusions. In case of questions or lack of any data, contact was made with the corresponding authors of the studies.
Study risk of bias assessment
The risk of bias in included studies was assessed using the Joanna Briggs Institute’s Critical Assessment Tool (14,15) for cohort studies. The tool consists of a checklist of 9 to 11 questions, where each one was judged with ‘yes’, ‘no’, ‘not clear’, and ‘not applicable’. The studies were characterized, regardless of the question asked, as high risk of bias when up to 49% of the answers are ‘YES’; moderate risk when between 50 and 69% of the answers are ‘YES’; and low risk when more than 70% of the answers are ‘YES’.
Synthesis methods
A qualitative analysis of the results was initially planned, considering the described data in frequency (%) of PCB self-correction during the transition of the dentitions; frequency of habits at the beginning and the end of each study; and data on the association between oral habits and PCB self-correction. A meta-analysis would be performed if the selected studies presented methodological, clinical, and statistical homogeneity of the data.
Certainty assessment
The certainty of the evidence was assessed using the Grading of Recommendations, Assessment, Development, and Evaluations Pro software (GRADE) (GRADEpro, available at https://www.gradepro.org/) (16). The GRADE tool classifies as ‘not serious’, ‘severe’ and ‘very serious’ each of the five domains evaluated: study design, risk of bias, inconsistency, indirect evidence, and inaccuracy of articles. And so, the final classification of the quality of evidence is given in four levels: very low, low, moderate, and high.
The domains were evaluated on three different outcomes:
a) Self-correction of PCB in the transition from deciduous to mixed dentition;
b) Self-correction of PCB in the transition from mixed to permanent dentition;
c) Self-correction of PCB in the transition from deciduous to permanent dentition;
d) Association between oral habits and self-correction of PCB from deciduous to permanent dentition.
Results
Study selection
Searches in the databases identified 3045 references: PubMed (n = 1257), Web of Science (n = 331), Scopus (n = 1365), LILACS (n = 15), and LIVIVO (n = 77). After removing the duplicate, 852 studies remained. The search in the grey literature found 350 references: Google Scholar (n = 350) and Open Grey (n = 0). One study was identified by manual search. Finally, the reference lists of included articles were evaluated, and no studies were identified.
After reading titles and abstracts, 836 records were excluded. Sixteen studies were selected for full-text evaluation and application of eligibility criteria. Of these, 12 were excluded (Supplementary Table 2). The study identified by the manual search was included. Thus, seven studies (6,17–22) were selected for qualitative synthesis. The process of identification and selection of studies is described in the PRISMA flow diagram (Figure 1).
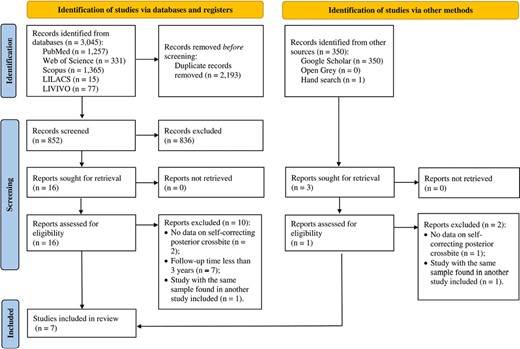
PRISMA flow diagram.
Study characteristics
Of the seven studies included, four studies (17,18,20,22) aimed to determine the occurrence of malocclusions, including PCB during the follow-up period. One study evaluated the need for orthodontic treatment in children with different types of malocclusions, including PCB (19). Finally, two studies evaluated early treatment of PCB compared to an untreated control group (6,21).
All included studies are cohort studies. Three of these studies evaluated the self-correction of PCB from deciduous to mixed dentition with a total sample of 149 patients, aged between 3 and 5 years at baseline (T0) (18,21,22). One study evaluated the presence of PCB self-correction from mixed to permanent dentition with a sample of 19 patients and a mean age of 7.7 years at T0 (19). The three remaining studies investigated the self-correction of PCB in the transition from deciduous to permanent dentition (6,17,20). The total sample includes 77 patients aged between 3 and 5 years at T0. The follow-up of the included studies was 5 (18,21,22), 8 (6,19), 8.5 (17), and 10 (20) years. The diagnostic method used in the studies for the diagnosis of PCB was determined by the method of Bjoerk (17,23) and Foster & Hamilton (17,18,24), based on the presence of lateral deviation or superior occlusion (20), with the buccal cusp of the maxillary tooth occluding the inferior lingually (21), or on clinical assessment and physical examination of occlusal interference (6). Most studies did not clarify which criterion was used to define self-correction of posterior crossbite (6,18–21), leaving it to appear that self-correction was observed by making a comparison with the findings obtained at T0. However, when we contacted the corresponding authors of the studies (17,18,22), two responded. The first reported that self-correction of posterior crossbite was observed when there was a normal eruption of the first permanent molar in the correct position (22). The second reported that self-correction was defined when the first permanent molar and premolars erupted into a normal transverse relationship at 11.5 years of age (17).
All included studies reported the presence of oral habits at T0, except for two. In one the oral habit had ceased before the start of the evaluation (21), and in the other study, there was no evaluation of oral habits (22). The summary of data from the included studies is described in Table 1.
Summary of the data from included studies.
| Authorship | Material | Methodology | Results | Conclusion | ||
|---|---|---|---|---|---|---|
| Sample characteristic | Exposure | |||||
| Author, year. Study design. | n (M/F) Age at T0 Evaluated dentition (follow-up) | Posterior crossbite classification Presence of oral habits | Diagnosis of posterior crossbite Statistical analysis | Diagnosis of self-correction of posterior crossbite. | Self-correction of posterior crossbite (%) Association between the persistence of oral habits and self-correction of posterior crossbite | |
| Khda et al., 2022 (22). Cohort study. | 70 (29/41) 4–5 years Deciduous to mixed (5 years) | UPCB/BPCB (57/10) NR (3) Not evaluated. | NR. Descriptive statistics (%) | Normal eruption of the first permanent molar in a correct position. | 54 of 70 children (77.1%) Not evaluated. | Spontaneous correction of PCB from the deciduous to the mixed dentition occurs in more than three-quarters of children. |
| Góis et al., 2012 (18). Cohort study. | 41 (NR) 3–5 years Deciduous to mixed (5 years) | NR 34% | Foster and Hamilton. Chi-square test and Relative Risk. | NR | 5 of 41 children (12.2%) There was no association between the removal of the oral habit and self-correction of posterior crossbite. | Children with untreated PCB in the primary dentition have a 7× greater risk of maintaining malocclusion in the mixed dentition. |
| Lindner, 1989 (21). Cohort study. | 38 (NR) 4 years Deciduous to mixed (5 years) | UPCB Habit ceased prior to the beginning of the study. | Buccal cusp of maxillary teeth occluding lingually to those of mandibular teeth. t test. | NR | 6 of 38 children (17% self-correction). Habit ceased prior to the beginning of the study. | Posterior crossbite does not appear to be self-correcting in the transition from deciduous to mixed dentition. |
| Heikinheimo et al., 1987 (19). Cohort study. | 19 (9/10) 7 years Mixed to permanent (8 years) | NR 1.5% | NR. Descriptive statistics (%). | NR | 3 of 19 children (15.7% self-correction). Not evaluated. | Posterior crossbite can self-correct in about 16% of cases during the eruption of permanent teeth. |
| Dimberg et al., 2015 (17). Cohort study. | 29 (NR) 3 years Deciduous to permanent (8.5 years) | UPCB 82% | Bjoerk and Foster & Hamilton. Chi-square test, odds ratio and McNamara’s test. | First permanent molar and the bicuspids erupted in a normal transversal relation. | 24 of 29 children (82.8% self-correction). 0.4% habit at T1, with no association with malocclusion. | UPCB self-correction in the primary dentition occurs in about 82% of cases and is not associated with the presence of the habit. |
| Kurol and Berglund, 1992 (20). Cohort study. | 20 (NR) 3-5 years Deciduous to permanent (10 years) | True or functional UPCB and unilateral or bilateral top bite 15.5% | Side deviation or edge-to-edge bite. Descriptive statistics (%). | NR | 4 of 20 children (20% self-correction). No oral habit was detected in T1. | Self-correction of posterior crossbite can occur up to 20% of patients in the transition from deciduous to permanent dentition. |
| Thilander et al.,1984 (6). Cohort study. | 28(11/17) 5 years Deciduous to permanent (8 years) | BPCB/UPCB 35.7% | Clinical evaluation, including examination of occlusal interferences. Descriptive statistics (%). | NR | 6 of 28 children (21.4% self-correction). There was no persistence of oral habits, or differences in the prevalence of habits between patients with or without spontaneous correction of crossbite. | Self-correction of posterior crossbite in the primary dentition may be as frequent as correction by occlusal adjustment. |
| Authorship | Material | Methodology | Results | Conclusion | ||
|---|---|---|---|---|---|---|
| Sample characteristic | Exposure | |||||
| Author, year. Study design. | n (M/F) Age at T0 Evaluated dentition (follow-up) | Posterior crossbite classification Presence of oral habits | Diagnosis of posterior crossbite Statistical analysis | Diagnosis of self-correction of posterior crossbite. | Self-correction of posterior crossbite (%) Association between the persistence of oral habits and self-correction of posterior crossbite | |
| Khda et al., 2022 (22). Cohort study. | 70 (29/41) 4–5 years Deciduous to mixed (5 years) | UPCB/BPCB (57/10) NR (3) Not evaluated. | NR. Descriptive statistics (%) | Normal eruption of the first permanent molar in a correct position. | 54 of 70 children (77.1%) Not evaluated. | Spontaneous correction of PCB from the deciduous to the mixed dentition occurs in more than three-quarters of children. |
| Góis et al., 2012 (18). Cohort study. | 41 (NR) 3–5 years Deciduous to mixed (5 years) | NR 34% | Foster and Hamilton. Chi-square test and Relative Risk. | NR | 5 of 41 children (12.2%) There was no association between the removal of the oral habit and self-correction of posterior crossbite. | Children with untreated PCB in the primary dentition have a 7× greater risk of maintaining malocclusion in the mixed dentition. |
| Lindner, 1989 (21). Cohort study. | 38 (NR) 4 years Deciduous to mixed (5 years) | UPCB Habit ceased prior to the beginning of the study. | Buccal cusp of maxillary teeth occluding lingually to those of mandibular teeth. t test. | NR | 6 of 38 children (17% self-correction). Habit ceased prior to the beginning of the study. | Posterior crossbite does not appear to be self-correcting in the transition from deciduous to mixed dentition. |
| Heikinheimo et al., 1987 (19). Cohort study. | 19 (9/10) 7 years Mixed to permanent (8 years) | NR 1.5% | NR. Descriptive statistics (%). | NR | 3 of 19 children (15.7% self-correction). Not evaluated. | Posterior crossbite can self-correct in about 16% of cases during the eruption of permanent teeth. |
| Dimberg et al., 2015 (17). Cohort study. | 29 (NR) 3 years Deciduous to permanent (8.5 years) | UPCB 82% | Bjoerk and Foster & Hamilton. Chi-square test, odds ratio and McNamara’s test. | First permanent molar and the bicuspids erupted in a normal transversal relation. | 24 of 29 children (82.8% self-correction). 0.4% habit at T1, with no association with malocclusion. | UPCB self-correction in the primary dentition occurs in about 82% of cases and is not associated with the presence of the habit. |
| Kurol and Berglund, 1992 (20). Cohort study. | 20 (NR) 3-5 years Deciduous to permanent (10 years) | True or functional UPCB and unilateral or bilateral top bite 15.5% | Side deviation or edge-to-edge bite. Descriptive statistics (%). | NR | 4 of 20 children (20% self-correction). No oral habit was detected in T1. | Self-correction of posterior crossbite can occur up to 20% of patients in the transition from deciduous to permanent dentition. |
| Thilander et al.,1984 (6). Cohort study. | 28(11/17) 5 years Deciduous to permanent (8 years) | BPCB/UPCB 35.7% | Clinical evaluation, including examination of occlusal interferences. Descriptive statistics (%). | NR | 6 of 28 children (21.4% self-correction). There was no persistence of oral habits, or differences in the prevalence of habits between patients with or without spontaneous correction of crossbite. | Self-correction of posterior crossbite in the primary dentition may be as frequent as correction by occlusal adjustment. |
BPCB, bilateral posterior crossbite; F, female; n, sample size; M, male; NR, not reported; PCB, posterior crossbite; UPCB, unilateral posterior crossbite; %, frequency; T0, initial assessment; T1, final assessment.
Summary of the data from included studies.
| Authorship | Material | Methodology | Results | Conclusion | ||
|---|---|---|---|---|---|---|
| Sample characteristic | Exposure | |||||
| Author, year. Study design. | n (M/F) Age at T0 Evaluated dentition (follow-up) | Posterior crossbite classification Presence of oral habits | Diagnosis of posterior crossbite Statistical analysis | Diagnosis of self-correction of posterior crossbite. | Self-correction of posterior crossbite (%) Association between the persistence of oral habits and self-correction of posterior crossbite | |
| Khda et al., 2022 (22). Cohort study. | 70 (29/41) 4–5 years Deciduous to mixed (5 years) | UPCB/BPCB (57/10) NR (3) Not evaluated. | NR. Descriptive statistics (%) | Normal eruption of the first permanent molar in a correct position. | 54 of 70 children (77.1%) Not evaluated. | Spontaneous correction of PCB from the deciduous to the mixed dentition occurs in more than three-quarters of children. |
| Góis et al., 2012 (18). Cohort study. | 41 (NR) 3–5 years Deciduous to mixed (5 years) | NR 34% | Foster and Hamilton. Chi-square test and Relative Risk. | NR | 5 of 41 children (12.2%) There was no association between the removal of the oral habit and self-correction of posterior crossbite. | Children with untreated PCB in the primary dentition have a 7× greater risk of maintaining malocclusion in the mixed dentition. |
| Lindner, 1989 (21). Cohort study. | 38 (NR) 4 years Deciduous to mixed (5 years) | UPCB Habit ceased prior to the beginning of the study. | Buccal cusp of maxillary teeth occluding lingually to those of mandibular teeth. t test. | NR | 6 of 38 children (17% self-correction). Habit ceased prior to the beginning of the study. | Posterior crossbite does not appear to be self-correcting in the transition from deciduous to mixed dentition. |
| Heikinheimo et al., 1987 (19). Cohort study. | 19 (9/10) 7 years Mixed to permanent (8 years) | NR 1.5% | NR. Descriptive statistics (%). | NR | 3 of 19 children (15.7% self-correction). Not evaluated. | Posterior crossbite can self-correct in about 16% of cases during the eruption of permanent teeth. |
| Dimberg et al., 2015 (17). Cohort study. | 29 (NR) 3 years Deciduous to permanent (8.5 years) | UPCB 82% | Bjoerk and Foster & Hamilton. Chi-square test, odds ratio and McNamara’s test. | First permanent molar and the bicuspids erupted in a normal transversal relation. | 24 of 29 children (82.8% self-correction). 0.4% habit at T1, with no association with malocclusion. | UPCB self-correction in the primary dentition occurs in about 82% of cases and is not associated with the presence of the habit. |
| Kurol and Berglund, 1992 (20). Cohort study. | 20 (NR) 3-5 years Deciduous to permanent (10 years) | True or functional UPCB and unilateral or bilateral top bite 15.5% | Side deviation or edge-to-edge bite. Descriptive statistics (%). | NR | 4 of 20 children (20% self-correction). No oral habit was detected in T1. | Self-correction of posterior crossbite can occur up to 20% of patients in the transition from deciduous to permanent dentition. |
| Thilander et al.,1984 (6). Cohort study. | 28(11/17) 5 years Deciduous to permanent (8 years) | BPCB/UPCB 35.7% | Clinical evaluation, including examination of occlusal interferences. Descriptive statistics (%). | NR | 6 of 28 children (21.4% self-correction). There was no persistence of oral habits, or differences in the prevalence of habits between patients with or without spontaneous correction of crossbite. | Self-correction of posterior crossbite in the primary dentition may be as frequent as correction by occlusal adjustment. |
| Authorship | Material | Methodology | Results | Conclusion | ||
|---|---|---|---|---|---|---|
| Sample characteristic | Exposure | |||||
| Author, year. Study design. | n (M/F) Age at T0 Evaluated dentition (follow-up) | Posterior crossbite classification Presence of oral habits | Diagnosis of posterior crossbite Statistical analysis | Diagnosis of self-correction of posterior crossbite. | Self-correction of posterior crossbite (%) Association between the persistence of oral habits and self-correction of posterior crossbite | |
| Khda et al., 2022 (22). Cohort study. | 70 (29/41) 4–5 years Deciduous to mixed (5 years) | UPCB/BPCB (57/10) NR (3) Not evaluated. | NR. Descriptive statistics (%) | Normal eruption of the first permanent molar in a correct position. | 54 of 70 children (77.1%) Not evaluated. | Spontaneous correction of PCB from the deciduous to the mixed dentition occurs in more than three-quarters of children. |
| Góis et al., 2012 (18). Cohort study. | 41 (NR) 3–5 years Deciduous to mixed (5 years) | NR 34% | Foster and Hamilton. Chi-square test and Relative Risk. | NR | 5 of 41 children (12.2%) There was no association between the removal of the oral habit and self-correction of posterior crossbite. | Children with untreated PCB in the primary dentition have a 7× greater risk of maintaining malocclusion in the mixed dentition. |
| Lindner, 1989 (21). Cohort study. | 38 (NR) 4 years Deciduous to mixed (5 years) | UPCB Habit ceased prior to the beginning of the study. | Buccal cusp of maxillary teeth occluding lingually to those of mandibular teeth. t test. | NR | 6 of 38 children (17% self-correction). Habit ceased prior to the beginning of the study. | Posterior crossbite does not appear to be self-correcting in the transition from deciduous to mixed dentition. |
| Heikinheimo et al., 1987 (19). Cohort study. | 19 (9/10) 7 years Mixed to permanent (8 years) | NR 1.5% | NR. Descriptive statistics (%). | NR | 3 of 19 children (15.7% self-correction). Not evaluated. | Posterior crossbite can self-correct in about 16% of cases during the eruption of permanent teeth. |
| Dimberg et al., 2015 (17). Cohort study. | 29 (NR) 3 years Deciduous to permanent (8.5 years) | UPCB 82% | Bjoerk and Foster & Hamilton. Chi-square test, odds ratio and McNamara’s test. | First permanent molar and the bicuspids erupted in a normal transversal relation. | 24 of 29 children (82.8% self-correction). 0.4% habit at T1, with no association with malocclusion. | UPCB self-correction in the primary dentition occurs in about 82% of cases and is not associated with the presence of the habit. |
| Kurol and Berglund, 1992 (20). Cohort study. | 20 (NR) 3-5 years Deciduous to permanent (10 years) | True or functional UPCB and unilateral or bilateral top bite 15.5% | Side deviation or edge-to-edge bite. Descriptive statistics (%). | NR | 4 of 20 children (20% self-correction). No oral habit was detected in T1. | Self-correction of posterior crossbite can occur up to 20% of patients in the transition from deciduous to permanent dentition. |
| Thilander et al.,1984 (6). Cohort study. | 28(11/17) 5 years Deciduous to permanent (8 years) | BPCB/UPCB 35.7% | Clinical evaluation, including examination of occlusal interferences. Descriptive statistics (%). | NR | 6 of 28 children (21.4% self-correction). There was no persistence of oral habits, or differences in the prevalence of habits between patients with or without spontaneous correction of crossbite. | Self-correction of posterior crossbite in the primary dentition may be as frequent as correction by occlusal adjustment. |
BPCB, bilateral posterior crossbite; F, female; n, sample size; M, male; NR, not reported; PCB, posterior crossbite; UPCB, unilateral posterior crossbite; %, frequency; T0, initial assessment; T1, final assessment.
Risk of bias in studies
Among the included studies, two had a low risk of bias (17,18), three had a moderate risk of bias (6,21,22) and two had a high risk of bias (19,20) according to the Joanna Briggs Institute checklist for cohort studies. Studies with low risk of bias did not show significant methodological bias. High-risk studies presented limitations in sample selection and uncertainties in exposure measurements, outcome evaluation, and statistical analysis performed. The three studies with moderate risk of bias have uncertainties in exposure measurements and identification of confounding factors. The results of the risk of bias assessment of the studies are shown in Figure 2.
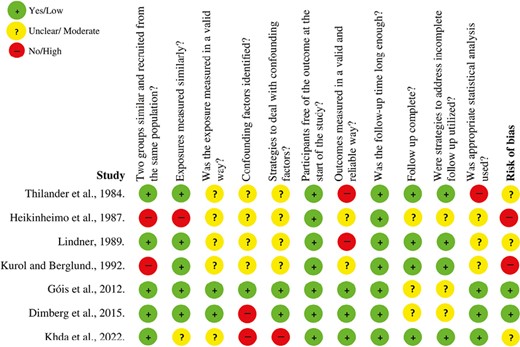
Risk of bias in included studies.
Results of individual studies
The study that evaluated the self-correction of PCB from mixed to permanent dentition found self-correction in three (15.7%) of the 19 children with untreated PCB (19). Regarding the studies that evaluated untreated PCB from deciduous to mixed dentition, one showed a self-correction of 12.2% (18), 5 of 41 untreated children. A study identified spontaneous correction in 6 of the 38 children studied, resulting in a self-correction of 17% (21). The other study exhibited a self-correction of 77.1%, corresponding to self-correction in 54 of the 70 untreated children (22). Therefore, in a pooled analysis, from deciduous to mixed dentition, self-correction occurred with an average frequency of about 43.6%, or in 65 of 149 children followed.
Three studies followed PCB in the transition from deciduous to permanent dentition. They found self-correction rates of 20% (20), 21.4% (6), and 82.8% (17). These data corresponded to a sample of 20, 28, and 29 untreated children with PCB, respectively. In addition to self-correction, other patients showed improvement in malocclusion. In a sample of 20 patients, four showed complete self-correction and another five showed improvements changing from a posterior crossbite condition to an edge-to-edge occlusal relationship (20). In another sample of 28 patients, in addition to the 6 who had complete self-correction, another 14 also showed improvement in their malocclusion (6).
Regarding oral habits, one study reported a PCB self-correction of 17% from deciduous to mixed dentition in patients who interrupted the oral habits previously found at the start of the study and before four years old (21). Of the five studies that reported the presence of oral habits at T0 (6,17–20), only one was not assessed in the final exam (T1) (19). Of the three studies that evaluated patients with this malocclusion from deciduous to permanent dentition, one showed data on the persistence of 0.4% of oral habits at the final assessment, compared to 82% at T0 (17). The other two studies observed that there was no persistence of the oral habit at T1, compared to a frequency of 15.5% (20) and 35.7% (6) at T0.
Regarding the association between oral habits and self-correction of PCB, three studies reported that there was no association between the persistence of oral habits and self-correction of PCB. One study evaluated patients with PCB from deciduous to mixed dentition (18), and the other two investigated from deciduous to permanent dentition (6,17). The study that evaluated PCB patients from mixed to permanent dentition did not assess the relationship between the persistence of oral habits and PCB self-correction (19).
Results of syntheses
Data from the included studies were qualitatively evaluated using PCB self-correction values described in frequency (%). The included studies showed sample differences regarding the classification of PCB, the diagnostic method, and the statistical analysis used. Due to this heterogeneity, it was not possible to perform a quantitative analysis.
Certainty of evidence
The level of certainty of the evidence of the occurrence of PCB self-correction in the transition from deciduous to mixed dentition was considered moderate and clinically important. One of the studies included in this analysis has a low risk of bias (18), and the other two have a moderate risk (21,22), due to limitations in the reliability of measuring exposures and outcomes. In relation to self-correction of PCB from mixed to permanent dentition, the evidence generated was very low, as the only study evaluated in this evidence (19) has a high risk of bias, with limitations in sample selection, reliability of measuring exposures and outcomes, as well as incomplete information about the follow-up and the statistical analysis used. Regarding PCB self-correction from the primary to permanent dentition, the evidence generated was low but clinically important, as this evidence can prevent overtreatment in childhood. Among the three studies evaluated, one had a low risk of bias (17), another had a moderate risk (6), and the other was classified as having a high risk (20), given its limitations in sample selection, reliability of exposition and evaluation of the results.
The relationship between the interruption of oral habits and PCB self-correction from deciduous to permanent dentition generated evidence with a low level of certainty. The studies analysed in this outcome (6,17,20) showed relatively high frequencies of oral habits in the deciduous dentition, up to 82% at T0 (17). On the other hand, in the final evaluation, the oral habit was detected in only 0.4% of the children. However, statistical analysis showed no association between habit removal and crossbite self-correction.
The assessment of the certainty of evidence according to the GRADE tool is described in Table 2.
GRADE analysis.
| Assessment of certainty | Impact | Certainty | ||||||
|---|---|---|---|---|---|---|---|---|
| № of studies | Study design | Risk of bias | Inconsistency | Indirect evidence | Imprecision | Other considerations | ||
| Self-correction of posterior crossbite in the transition from deciduous to mixed dentition | ||||||||
| 3 | Observational study | Not serious | Not serious | Not serious | Not serious | Not detected | Studies by Khda, et al., 2022; Góis et al., 2012 and Lindner, 1989 report that between 12.2 and 77.1% of posterior crossbite cases in the primary dentition will self-correct in the mixed dentition. | ⊕⊕⊕◯ MODERATE |
| Self-correction of posterior crossbite in the transition from mixed to permanent dentition | ||||||||
| 1 | Observational study | Very seriousa | Not serious | Not serious | Not serious | Not detected | The study by Heikinheimo et al., 1987 reported that self-correction of posterior crossbite can occur in up to 15.7% of cases during the transition from mixed to permanent dentition. | ⊕◯◯◯ VERY LOW |
| Self-correction of posterior crossbite in the transition from deciduous to permanent dentition | ||||||||
| 3 | Observational study | Seriousb | Not serious | Not serious | Not serious | Not detected | Three studies (Dimberg et al., 2015; Kurol and Berglund, 1992 and Thilander et al., 1984) state that between 20 and 82.8% of children in the primary dentition with posterior crossbite will self-correct this malocclusion in the permanent dentition. | ⊕⊕◯◯ LOW |
| Association between oral habits and posterior crossbite self-correction in the transition from deciduous to permanent dentition | ||||||||
| 3 | Observational study | Seriousc | Not serious | Not serious | Not serious | Not detected | The oral habit was detected in only 0.4% of children in the transition from deciduous to mixed dentition, based on the evaluation of three studies (Dimberg et al., 2015; Kurol and Berglund, 1992 and Thilander et al., 1984). | ⊕⊕◯◯ LOW |
| Assessment of certainty | Impact | Certainty | ||||||
|---|---|---|---|---|---|---|---|---|
| № of studies | Study design | Risk of bias | Inconsistency | Indirect evidence | Imprecision | Other considerations | ||
| Self-correction of posterior crossbite in the transition from deciduous to mixed dentition | ||||||||
| 3 | Observational study | Not serious | Not serious | Not serious | Not serious | Not detected | Studies by Khda, et al., 2022; Góis et al., 2012 and Lindner, 1989 report that between 12.2 and 77.1% of posterior crossbite cases in the primary dentition will self-correct in the mixed dentition. | ⊕⊕⊕◯ MODERATE |
| Self-correction of posterior crossbite in the transition from mixed to permanent dentition | ||||||||
| 1 | Observational study | Very seriousa | Not serious | Not serious | Not serious | Not detected | The study by Heikinheimo et al., 1987 reported that self-correction of posterior crossbite can occur in up to 15.7% of cases during the transition from mixed to permanent dentition. | ⊕◯◯◯ VERY LOW |
| Self-correction of posterior crossbite in the transition from deciduous to permanent dentition | ||||||||
| 3 | Observational study | Seriousb | Not serious | Not serious | Not serious | Not detected | Three studies (Dimberg et al., 2015; Kurol and Berglund, 1992 and Thilander et al., 1984) state that between 20 and 82.8% of children in the primary dentition with posterior crossbite will self-correct this malocclusion in the permanent dentition. | ⊕⊕◯◯ LOW |
| Association between oral habits and posterior crossbite self-correction in the transition from deciduous to permanent dentition | ||||||||
| 3 | Observational study | Seriousc | Not serious | Not serious | Not serious | Not detected | The oral habit was detected in only 0.4% of children in the transition from deciduous to mixed dentition, based on the evaluation of three studies (Dimberg et al., 2015; Kurol and Berglund, 1992 and Thilander et al., 1984). | ⊕⊕◯◯ LOW |
aThe study has a high risk of bias; bOne study had a high risk of bias; cOne study had a high risk of bias.
GRADE analysis.
| Assessment of certainty | Impact | Certainty | ||||||
|---|---|---|---|---|---|---|---|---|
| № of studies | Study design | Risk of bias | Inconsistency | Indirect evidence | Imprecision | Other considerations | ||
| Self-correction of posterior crossbite in the transition from deciduous to mixed dentition | ||||||||
| 3 | Observational study | Not serious | Not serious | Not serious | Not serious | Not detected | Studies by Khda, et al., 2022; Góis et al., 2012 and Lindner, 1989 report that between 12.2 and 77.1% of posterior crossbite cases in the primary dentition will self-correct in the mixed dentition. | ⊕⊕⊕◯ MODERATE |
| Self-correction of posterior crossbite in the transition from mixed to permanent dentition | ||||||||
| 1 | Observational study | Very seriousa | Not serious | Not serious | Not serious | Not detected | The study by Heikinheimo et al., 1987 reported that self-correction of posterior crossbite can occur in up to 15.7% of cases during the transition from mixed to permanent dentition. | ⊕◯◯◯ VERY LOW |
| Self-correction of posterior crossbite in the transition from deciduous to permanent dentition | ||||||||
| 3 | Observational study | Seriousb | Not serious | Not serious | Not serious | Not detected | Three studies (Dimberg et al., 2015; Kurol and Berglund, 1992 and Thilander et al., 1984) state that between 20 and 82.8% of children in the primary dentition with posterior crossbite will self-correct this malocclusion in the permanent dentition. | ⊕⊕◯◯ LOW |
| Association between oral habits and posterior crossbite self-correction in the transition from deciduous to permanent dentition | ||||||||
| 3 | Observational study | Seriousc | Not serious | Not serious | Not serious | Not detected | The oral habit was detected in only 0.4% of children in the transition from deciduous to mixed dentition, based on the evaluation of three studies (Dimberg et al., 2015; Kurol and Berglund, 1992 and Thilander et al., 1984). | ⊕⊕◯◯ LOW |
| Assessment of certainty | Impact | Certainty | ||||||
|---|---|---|---|---|---|---|---|---|
| № of studies | Study design | Risk of bias | Inconsistency | Indirect evidence | Imprecision | Other considerations | ||
| Self-correction of posterior crossbite in the transition from deciduous to mixed dentition | ||||||||
| 3 | Observational study | Not serious | Not serious | Not serious | Not serious | Not detected | Studies by Khda, et al., 2022; Góis et al., 2012 and Lindner, 1989 report that between 12.2 and 77.1% of posterior crossbite cases in the primary dentition will self-correct in the mixed dentition. | ⊕⊕⊕◯ MODERATE |
| Self-correction of posterior crossbite in the transition from mixed to permanent dentition | ||||||||
| 1 | Observational study | Very seriousa | Not serious | Not serious | Not serious | Not detected | The study by Heikinheimo et al., 1987 reported that self-correction of posterior crossbite can occur in up to 15.7% of cases during the transition from mixed to permanent dentition. | ⊕◯◯◯ VERY LOW |
| Self-correction of posterior crossbite in the transition from deciduous to permanent dentition | ||||||||
| 3 | Observational study | Seriousb | Not serious | Not serious | Not serious | Not detected | Three studies (Dimberg et al., 2015; Kurol and Berglund, 1992 and Thilander et al., 1984) state that between 20 and 82.8% of children in the primary dentition with posterior crossbite will self-correct this malocclusion in the permanent dentition. | ⊕⊕◯◯ LOW |
| Association between oral habits and posterior crossbite self-correction in the transition from deciduous to permanent dentition | ||||||||
| 3 | Observational study | Seriousc | Not serious | Not serious | Not serious | Not detected | The oral habit was detected in only 0.4% of children in the transition from deciduous to mixed dentition, based on the evaluation of three studies (Dimberg et al., 2015; Kurol and Berglund, 1992 and Thilander et al., 1984). | ⊕⊕◯◯ LOW |
aThe study has a high risk of bias; bOne study had a high risk of bias; cOne study had a high risk of bias.
Discussion
The data collected demonstrate that self-correction of PCB in childhood is possible, with an occurrence between 12.2 (18) and 82.8% (17) of children, varying according to the period of dental transition evaluated. From deciduous to mixed dentition, there was an occurrence of 12.2 (18) to 77.1% (22) of self-correction among the 149 children evaluated, with moderate evidence. From deciduous to permanent dentition, self-correction values ranged from 20 (20) to 82.8% (17), with a low level of certainty of evidence. Frequency differences between these studies may be related to the type of diagnostic method used to assess PCB. Furthermore, these statistical differences may be associated with the possibility that some permanent teeth erupt in a normal position, replacing the crossed deciduous teeth during dental changes. Also, the literature presents studies that reaffirm that PCB doesn’t present self-correction (9,10,25), as they did not find cases of self-correction among their patients with untreated PCB. However, these studies observed patients for a short period of follow-up (±1 year) and evaluated these patients in specific dentitions (deciduous or mixed). Therefore, it seems suggestive that the follow-up of patients during the different stages of dentition is essential for the analysis of data regarding PCB self-correction.
Even separating by evaluated dentition transition, the self-correction frequencies demonstrate group heterogeneity. Ranging from 12.2 (18) to 77.1% (22) in the transition from deciduous to mixed dentition and from 20 (20) to 82.8% (17) in the transition from deciduous to permanent dentition. A justification for this discrepancy between self-correction percentages could be the risk of bias in each included study. However, the two highest percentages of self-correction found (82% and 77%) are in studies with low (17) and moderate (22) risk of bias. The same is observed among the lowest self-correction percentages, where the study with 12.2% of PCB self-correction (18) has a low risk of bias, the study with 15.7% (19) has a high risk, and the study with 17% (21) has a risk of moderate bias. Therefore, it is not possible to state that the heterogeneity of these PCB self-correction percentages may be associated with the risk of bias of the included studies.
Previous systematic reviews have already addressed data on self-correction of PCB (26,27). The first assessed how orthodontic treatments can affect unilateral PCB from deciduous to early mixed dentition and concluded that this malocclusion does not have spontaneous correction, therefore, its correction requires the use of orthodontic appliances (26). Another systematic review evaluated the occurrence of self-correction of malocclusions after removing non-nutritive sucking habits (27). This study reported that spontaneous PCB correction rarely occurs and that habit removal doesn’t appear to increase the likelihood of self-correction after 4 years of age. With the exception of one study (17), both reviews included studies with a short follow-up to evaluate patients with PCB, demonstrating that a longer follow-up is probably necessary to evaluate the self-correction of this malocclusion.
The studies included in this research that evaluated PCB from the deciduous to permanent dentition (6,17,20) conclude that self-correction is possible in 20 (20) to 82% (17) of patients. These studies showed high frequencies of self-correction and also higher frequencies of children who abandoned the habit during the follow-up period, with a frequency of 0.4% of habit persistence at T1. However, the data collected in this research do not allow inferring that the removal of the oral habit can motivate PCB self-correction.
Most of the studies included in this research did not adequately report the PCB diagnosis method or whether the patients were examined in occlusion in maximum habitual intercuspation or in centric relation, as well as the classification of PCB severity. Since the distinction between unilateral or bilateral PCB and also the distinction between functional, dental, or skeletal PCB can be factors influencing self-correction, these characteristics should be reported. Malocclusions of dental origin and with few teeth involved could have a better prognosis and a greater tendency to self-correction, unlike those of skeletal origin, which often have an unfavourable prognosis.
It is also important to note that only two studies (17,22) provided information on the criteria used to define self-correction of posterior crossbite. For the other studies, where this information was not obtained (6,18–21), there is no way to know precisely the degree of improvement or degree of self-correction of patients with a posterior crossbite. In addition, some studies reported cases of malocclusion improvement (6) and cases of patients who went from a posterior crossbite condition to an edge-to-edge relationship (20); however, both studies also did not report the criteria used to define such an improvement. Therefore, in addition to describing in detail the severity and classification of malocclusion, it seems suggestive that future studies begin to describe a criterion to define self-correction of posterior crossbite. This information can significantly influence the final percentage of posterior crossbite cases classified as self-correcting.
Previous studies showed that children with PCB may present asymmetrical muscle activity during mastication or clenching, increasing the likelihood of them developing signs and symptoms of temporomandibular disorders (7). This systematic review did not find data that can accurately identify which children with PCB may undergo self-correction. In this sense, the appropriate treatment for each child must be defined according to the orthodontic need based on a correct diagnosis of PCB. Functional consequences of this malocclusion for the growth and development of the stomatognathic system should also be taken into account.
Studies with methodological accuracy on the self-correction of PCB are necessary, as well as the evaluation of the impact of oral habits and other predictors on this condition. Moreover, studies that classify samples according to the severity and different types of PCB are important to obtain reliable findings, approaching an accurate diagnosis to classify between unilateral or bilateral PCB and dental or skeletal PCB. This knowledge can change the mechanisms to treat paediatric patients with PCB, knowing that if the factors are identified that could result in the self-correction of PCB during tooth changes, early childhood orthodontic treatment can be postponed.
Limitations
The limitations of this systematic review are related to the observational design of some included studies, without adequate control for confounding factors; the non-classification of the samples considering the different types of PCB or the severity of the malocclusion, and the use of different ways of evaluating and diagnosing PCB.
Conclusions
Self-correction of PCB in childhood is possible.
The results of this research show that PCB self-correction in the transition from deciduous to mixed dentition is possible, based on moderate certainty evidence based on three studies with risk of bias ranging from moderate to low.
Only one study was used to analyse self-correction in the mixed to permanent dentition, resulting in very low evidence for this outcome.
The results show that self-correction in the transition from deciduous to permanent dentition is possible, but the level of certainty of the evidence was low.
It is not possible to infer that the discontinuity of oral habits in the deciduous and mixed dentition is associated with cases of PCB self-correction in the permanent dentition, according to the low level of evidence.
A great variability in the findings of the studies has been reported and the results of this research do not allow to state how often the self-correction of posterior crossbite occurs in childhood or in which period of the dentition this process is more likely to occur.
Funding
No funding was received for the research, authorship, and publication of this systematic review.
Author Contributions
Bianka Nascimento (Data curation-Equal, Investigation-Equal, Methodology-Equal, Writing – original draft-Lead, Writing – review & editing-Equal), Cibelle Santos (Formal analysis-Equal, Investigation-Equal, Methodology-Lead, Project administration-Equal, Supervision-Lead, Writing – original draft-Equal, Writing – review & editing-Equal), Milena Santos (Data curation-Supporting, Methodology-Supporting, Supervision-Supporting, Visualization-Supporting, Writing – original draft-Supporting, Writing – review & editing-Equal), David Normando (Conceptualization-Lead, Formal analysis-Lead, Methodology-Supporting, Project administration-Lead, Supervision-Lead, Validation-Lead, Writing – review & editing-Lead)
Conflicts of interest
The authors declare that there is no conflict of interest.
Data availability
The data underlying this article are available in the article and in its online supplementary material.


{kind=link}
{kind=link}