






Abstract
HEARTSTRING is a useful proximal anastomosis assist device, but it has a drawback in that the removal process is irreversible. If thread cutting occurs during the tying process, repair without side clamping is difficult. We developed a simple modified technique for the safe removal of the HEARTSTRING device.
INTRODUCTION
Several proximal anastomosis assist devices have been developed to avoid aortic clamping. PAS-Port (Dextera Surgical Inc., Redwood City, CA, USA) is an automated device designed exclusively for a saphenous vein graft. Enclose II (Vitalitec International Inc., Plymouth, MA, USA) provides. a secure anastomosis with hand sutures, but an additional puncture site is required. The HEARTSTRING III Proximal seal system (MAQUET Holding B.V. & Co. KG, Rastatt, Germany) also allows a hand-sewn anastomosis. Its drawback, however, is the irreversibility of device removal. The instructions for use of the device recommend tying of the thread after device removal. Accidental thread cutting is a very rare incidence; however, if it occurs, it requires extensive effort and side clamping to control bleeding. We report a new modified technique for safer removal of the HEARTSTRING device
TECHNIQUE
The HEARTSTRING III Aortic Cutter was used to punch out the aorta, followed by introduction of the HEARTSTRING III Proximal Seal System. The proximal anastomosis was secured using 6-0 polyvinylidene fluoride suture (Asflex; CrownJun Kono Corp., Tokyo, Japan) in a side-to-side manner, leaving at least 7 mm of remnant graft beyond the anastomosis site. Halfway through the suturing process, the anchor string of the device was cut at 1 cm from the anchor tab and passed inside the graft lumen to the free end (Fig. 1A). The anchor string was reattached with a Hemoclip (Teleflex Inc., Wayne, PA, USA) to prevent losing the device into the aorta and to restore the weight role of the anchor tab. After completing the remaining suturing, thread tying was accomplished. Finally, the HEARTSTRING was removed through the free end of the graft, vertically from the aorta (Fig. 1B). Because the free end was still open, we could easily remove the air or debris, if existent, by spouting them out with the blood stream. Bleeding from the free end was easily controlled with fingers. The free end was ligated twice, with medium-sized Hemoclips. The anastomosis was completed (Fig. 1C). In addition, our method is applicable for a piggyback anastomosis as shown in Fig. 1D.
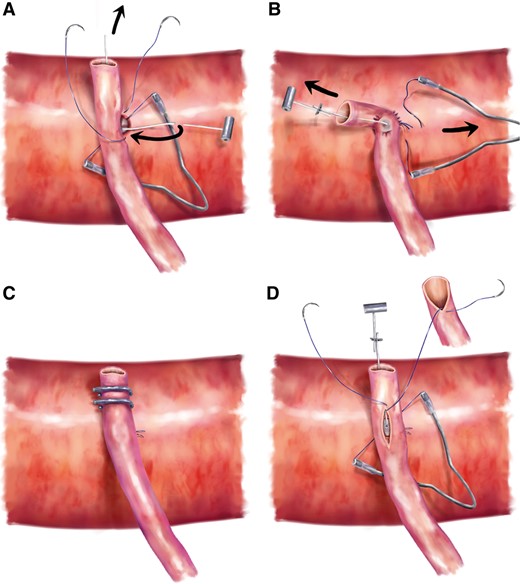
Schematic illustration of the anastomosis steps. (A) The graft is anastomosed to the ascending aorta in a side-to-side manner. Midway through the suturing, the anchor string of the HEARTSTRING is cut and passed inside the graft lumen to the free end. (B) After completion of suturing, the thread is tied. The HEARTSTRING device is removed through the free end of the graft. (C) The free end is ligated twice with medium-sized Hemoclips. The anastomosis is complete. (D) The point of a piggyback anastomosis is shown. The roof of the initially anastomosed graft was incised, and the second graft was anastomosed onto the roof of the primary graft.
Angiography or computed tomographic angiography was performed to assess the graft patency and shape of the anastomosis. A widely patent anastomosis with a smooth cobra head shape was seen (Fig. 2A and B).
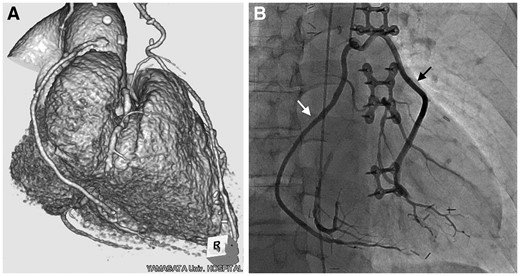
(A) Postoperative computed tomographic angiography of radial artery graft and (B) postoperative angiography of saphenous vein grafts anastomosed in a piggyback fashion are shown. White arrow indicates a graft to right coronary artery and black arrow indicates a graft to the circumflex artery.
COMMENTS
Because cases requiring coronary artery bypass grafting can often be critically complex, an increasing number of patients require multivessel bypass. Although the advantage of using the bilateral internal thoracic arteries has been reported [1], the need for aortocoronary bypass is still significant. Several proximal anastomosis assist devices have been developed to avoid aortic clamping. Among these, the HEARTSTRING is considered the most innocuous. However, this device has a drawback in that its removal process is irreversible. If thread cutting takes place, side clamping is necessary. Our simple technique can resolve the complication without a complex procedure.
An additional advantage of this method is its applicability for procedures involving multivessel composite grafts with a single proximal anastomosis [2–4]. Adopting our technique for these procedures would enable safer anastomosis and reduce costs.
We used this technique for 1 year, in 15 consecutive proximal anastomoses, including 4 piggyback anastomoses. No adverse events were observed. Because the follow-up period was short and the number of cases was limited, we plan to continue using the technique to accumulate more evidence.
In conclusion, our simple modification for the removal of the HEARTSTRING is beneficial and provides an excellent initial clinical outcome. This technique can be a useful alternative for the removal of the HEARTSTRING device.
ACKNOWLEDGEMENTS
The authors thank Kaoru Kikuyama for drawing the illustrations. We also thank Editage [www.editage.jp (15 July 2017, date last accessed)] for English language editing.
Conflict of interest: none declared.

{kind=link}
{kind=link}