






Abstract
Phaeochromocytoma is a rare catecholamine-secreting tumour involved in 0.1–0.2% cases of hypertension in the general population. Headache, palpitation and paroxystic sweating are the most commonly described symptoms. A few published cases report an acute adrenergic cardiomyopathy, leading to severe cardiogenic shock requiring mechanical circulatory support. We report the case of a 57-year old patient presenting a voluminous phaeochromocytoma of the left adrenal gland revealed by cardiogenic shock and rescued by peripheral extracorporeal life support device (ECLS). Left surrenalectomy has been performed under protective ECLS during the same surgical procedure. The patient was successfully weaned from ECLS on Day 7 after surgery and myocardial function completely recovered when the patient was discharged from the hospital.
CLINICAL SUMMARY
A 57-year old patient was referred to our hospital with brutal dyspnoea, abdominal pain, nausea and vomiting. He had no previously known pathology and his only cardiovascular risk factor was smoking. One of his aunts was operated for phaeochromocytoma. No headache, paroxystic tachycardia or sweating occurred before, but the patient suffered for 2 years of tiredness, anorexia, weight loss of 8 kg and recently permanent dysphagia. Initial blood pressure was 119/79 mmHg, body temperature was 36.5°C and his cardiac rate was 112 beat min −1 with no remarkable electrocardiographic abnormality. Arterial blood gases revealed a pH of 7.27, Po 2 of 80 mmHg (10.5 kPa), Pco 2 of 40 mmHg (5.2 kPa), bicarbonate of 28 mEq l −1 and lactate level of 3.3 mmol l −1 . Transthoracic echocardiography revealed a severe global left ventricular dysfunction, especially relaxation disorder, with a left ventricular ejection fraction (LVEF) of 20%. The left ventricular outflow tract velocity time integral (VTI) was 9 cm and the end-diastolic left ventricular diameter was 62 mm. First blood analyses showed moderate elevation of liver enzymes without liver dysfunction and moderate kidney failure. Early urinary concentrations of metanephrine and normetanephrine were respectively 100 µmol day −1 (normal: 0.35–1 μmol day −1 ) and 187 μmol day −1 (normal: 0.5–2 μmol day −1 ). Plasmatic measurements of renin and chromogranine A were respectively 470 μg l −1 (normal: <20 μg l −1 ) and 4951 ng l −1 (normal: <84.7 ng l −1 ). Emergency coronary arteriogram was performed and the patient’s coronary arteries were revealed. Subsequent abdominal computed tomography revealed a voluminous multilobar mass in the left adrenal gland, with a radiological aspect highly suggestive of phaeochromocytoma (Fig. 1 A and B), without secondary extension. After maximal medical treatment (intravenous α-blocker and calcic inhibitor), cardiogenic shock worsened in a few hours with LVEF of 10%, VTI of 6.5 cm and lactate level of 5.3 mmol l −1 . Femoro-femoral ECLS was initiated (Sorin® SCPC pump, Eos ECMO Sorin® oxygenator, Milan, Italy) and the concomitant removal of the voluminous phaeochromocytoma was performed under protective ELCS to allow myocardial full recovery by phaeochromocytoma resection. A bolus injection of 5000 IU of heparin was administered prior to ECLS implantation. Curative anticoagulation protocol with intravenous heparin was begun 6 h after surgery. The target range of anti-Xa activity was 0.2–0.3. Preventive anticoagulation protocol (10000 IU day −1 ) was followed as soon as the patient was weaned from ECLS. No complications occurred during the surgery, especially pump flow disorder (weight = 72 kg, height = 174 cm, body surface = 1.88 m 2 , theoretical pump outflow = 4.5 l min −1 ) or abnormal bleeding. Complete open left adrenalectomy was performed (Fig. 2 ). Myocardial recovery occurred on Day 4 and ECLS was discontinued on Day 7 after surgery, with LVEF of 30%. Nevertheless, a few complications occurred: 6 days after ECLS' withdrawal, a left retroperitoneal haematoma compressing the renal vessels occurred and led to surgical evacuation. Concomitant kidney failure required iterative intermittent dialysis sessions. A general sepsis also occurred because of the femoral cannulation. Infection was treated with adapted antibiotherapy and removal of the ECLS device at Day 7. Myocardial function completely recovered when the patient was discharged from the hospital, with LEVF of 50% and VTI of 18 cm and without kidney failure.
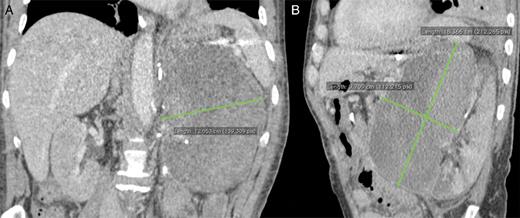
Contrasted abdominal computed tomography showing the voluminous left adrenal tumour.

Complete resection of the voluminous multilobar tumour (19 × 17 × 12.5 cm, 1754 kg) has been successfully performed by open surgery under protective extracorporeal life support device. Pheochromocytoma was confirmed by histological analysis with intense chromogranine A and synaptophysin immunolabelling.
DISCUSSION
Phaeochromocytomas are rare catecholaminergic-producing tumours with variable clinical presentations. Sudden cardiogenic shock can rarely occur as the first manifestation of the phaeochromocytoma [ 1 ]. Non-specific clinical presentations are also reported and are included in a pleomorphic syndrome such as abdominal pain, lumbar pain or multisystem organ failure syndrome (phaeochromocytoma multisystem crisis) [ 2 ]. Surgical timing is still not well established in patients with left ventricular severe dysfunction requiring mechanical support induced by phaeochromocytoma. Most of the reported cases were treated in two different steps: surgical adrenalectomy under open or ceolioscopic procedure a few days after haemodynamic stabilization and weaning from ECLS. To our knowledge, only 2 reported cases are operated under ECLS [ 3 , 4 ]. Ritter et al. [ 3 ] reported the case of a patient who underwent open right adrenalectomy under protective ECLS, which was removed immediately after resection during the same surgery. Grinda et al. [ 4 ] also reported the case of a patient presenting a refractory cardiogenic shock induced by phaeochromocytoma and massive pulmonary oedema. The surgical treatment of the tumour and placement of a left ventricular device (DeBakey axial pump) as bridge-to-bridge have been performed under protective ECLS. Besides, intra-aortic balloon pump was combined to ECLS in some cases [ 5 ]. In the present case, we performed peripheral ECLS and open adrenalectomy during the same surgery because of the great size of the tumour, considering that no myocardial recovery could be expected with such a catecholamine-secreting tumour. No ECLS pump disorder occurred during the surgical dissection of the vena cava and the left renal vein, but a compressing retroperitoneal haematoma led to surgical evacuation 6 days after ECLS' withdrawal. No distributive shock, due to the lack of pharmacological preparation, occurred after surgery.
In conclusion, a combined surgical strategy for catecholaminergic shock associating concomitant peripheral ECLS implantation and open adrenalectomy can be performed. This strategy must be reasonably considered because of the high risk of bleeding and ECLS outflow disorders.
Conflict of interest: none declared.
REFERENCES

{kind=link}
{kind=link}