






Despite advances in surgical techniques and postoperative medical management, the mortality rates for cardiac reoperations remain high. The risk is most commonly associated with failed resternotomy complicated by fatal injury to the myocardium or its structures. This short case report documents the first use of an endoluminal balloon occlusive device in order to prevent aneurysmal sack damage and coronary vessel injury in a patient with a giant aortic aneurysm after failed aortic surgery. The safe aortic occlusion allowed for closed-chest cardioplegia delivery and subsequent aortic unloading, thus facilitating a difficult but uneventful resternotomy.
INTRODUCTION
Despite advances in surgical techniques and postoperative medical management, the mortality rates for many different cardiac reoperations remain high. The risk is most commonly associated with failed resternotomy complicated by fatal injury to the myocardium or its structures [1]. We present a case of a third reoperation in a patient with a giant aneurysm of the sinuses of Valsalva, after previous replacement of the aortic valve and of the ascending aorta with an interposition graft. Owing to the severely enlarged aortic aneurysm adherent to the posterior surface of the sternum, an intravascular balloon clamping device was used.
CASE PRESENTATION
A 59-year old female was admitted to our Centre with mild, but progressive symptoms of congestive heart failure. In 1990, at the age of 36, she was diagnosed with severe aortic insufficiency and aortoannular ectasia. The valve was replaced with a mechanical St Jude 27 prosthesis, and the ascending aorta (52 mm) was longitudinally opened and plicated at a tertiary centre. The patient was readmitted to the same institution 3 years later for reoperation due to a non-dissecting giant (72 mm) aneurysm of the sinuses of Valsalva. The second surgical procedure (incomplete?) consisted of intra-aortic placement of the Dacron graft from the level of the sinotubular junction to a healthy part of the ascending aorta. The aneurysmal sack was wrapped around the prosthesis. Shortly after the procedure, the patient suffered from inferior myocardial infarction, but no coronary intervention was performed. No further information was available at the time of admission to our centre.
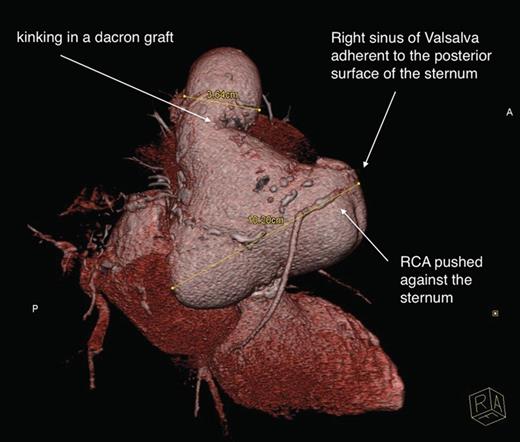
Severely enlarged aortic sinuses. Right coronary artery (RCA) modelled by the right aortic sinus.
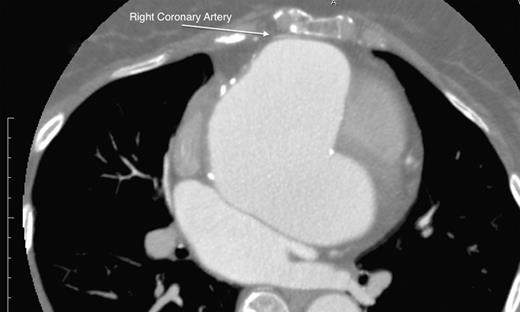
Right coronary artery adherent to the sternum, displaced by the enlarged right coronary sinus.
An intra-aortic occlusion device (IntraClude, Edwards, USA) was chosen as it offers a large soft elastomeric occlusive balloon with a large central lumen that delivers antegrade cardioplegia, and two smaller lines for venting and pressure monitoring. A dedicated inflow aortic cannula, equipped with a sidearm facilitating endoclamp placement (EndoReturn 21Fr, Edwards, USA) was used for femoral cannulation. The IntraClude was introduced into the ascending aorta over a guidewire. The safety point for aortic occlusion was marked by the visualization of the tip of the IntraClude catheter at the border zone of the aortic prosthesis and the aneurysmal sack. Arterial pressure was monitored by two independent lines in both radial arteries and was compared with the pressure in the aortic root. Once the position of the balloon was confirmed, its inflation began. Occlusion was recognized by a pressure drop in the aortic root and was confirmed by transesophageal echocardiography (TEE). Cardioplegia delivery was initiated (flow 300 ml/min, dose 2000 ml custodiol histidine-tryptophan-ketoglutarate) followed by aortic venting. Resternotomy with an oscillating sternal saw caused no injury to the aorta, myocardium or the surrounding structures. Full aortic root replacement was then performed with a modified composite graft. Since both coronaries were severely adherent to the surrounding tissue, they were reattached to the aortic graft with two separate 8 mm GoreTex grafts (modified Cabrol) so as to avoid kinking or malperfusion. The IntraClude was exchanged for a regular cross-clamp to facilitate distal aortic anastomosis. The patient's course was uneventful with fast recovery.
DISCUSSION
This short case report documents the first use of an endoluminal balloon occlusion device in order to prevent injury to the aneurysmal sack and coronary vessels in a patient with a giant aortic aneurysm after failed aortic surgery.
The formation of a pseudoaneurysm at the suture lines and progression of an aortic aneurysm are major problems in patients with a history of previous incomplete aortic aneurysm replacement [1]. Despite advances in surgical techniques and postoperative medical management, mortality rates remain high. The risk is most commonly associated with failed resternotomy complicated by fatal injury to the myocardium or its structures.
In the presented case, four surgical options were considered. The first was systemic cooling with femoral cannulation and resternotomy performed under deep hypothermic circulatory arrest. The second consisted in partial upper hemisternotomy, aortic cross-clamping and cardioplegia delivery with subsequent full sternotomy. The third option was based on carotid cannulation and full root replacement [2]. However, none of the proposed approaches could provide the unloading of the aneurysmal sack to prevent its injury. Hemisternotomy could potentially have lowered the risk of injury through aortic venting, but the process of resternotomy and aortic preparations would have been challenging. The fourth option was based on the assumption that the aorta can be clamped from the inside, and required the induction of myocardial arrest and effective aortic venting. While the Foley catheter has been proved to be effective in difficult patients, its introduction and application as effective venting/cardioplegia lines were doubtful [3]. The endoluminal balloon clamp has been used in a variety of minimally invasive, video-assisted cardiac procedures or in the presence of severe aortic calcifications. However, the initial enthusiasm was hampered by the incidence of iatrogenic aortic dissection resulting in a significantly higher risk of in-hospital death and a numerically higher risk of stroke [4]. An incomplete aortic occlusion was frequent, thus forcing balloon overinflation, which in turn could promote intimal tear, dissection or plaque disruption leading to peripheral or cerebral embolism. Other problems involved balloon protrusion and dislocation, often noticed in procedures requiring aortotomy.
The IntraClude may be free of the flaws present in the first generation, especially in terms of device positioning and the minimized risk of dislocation due to the modified anchoring system. Nevertheless, the general concept— of a balloon, remained unchanged, maintaining its previous flaws and imperfections amplifying the need for caution during inflation against the native aortic wall. Indeed, the device should not be used in severe aortic atherosclerosis.
In the described case, the device was easily positioned within the Dacron graft. By avoiding the native aorta and the aneurysm, extensive inflation was achieved, providing excellent occlusion, fast myocardial arrest and effective venting. In cases of aortic valve insufficiency, hypothermia-induced ventricular fibrillation should trigger balloon inflation, while venting would lead to aneurysmal sack decompression. Immediate cardioplegia delivery should be commenced once the aorta has been opened.
Although balloon visualization under fluoroscopy was also considered, especially with a hybrid room available, TEE was found much more versatile and user-friendly.
In conclusion, an intraluminal balloon occlusion device can be effectively used to clamp the ascending aorta in difficult cardiac reoperation, especially if the Dacron graft was used previously.
Conflict of interest: none declared.

{kind=link}