






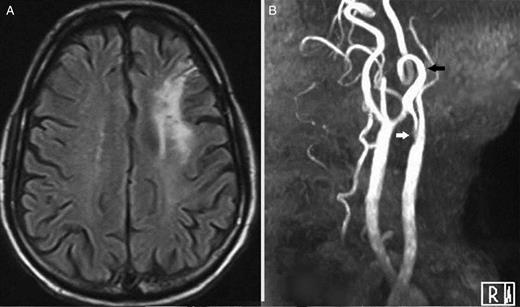
(A) Brain magnetic resonance imaging axial fluid-attenuated inversion recovery image demonstrating hyperintensity in the left fronto-parietal region suggestive of infarct. This patient had recurrent transient right upper limb monoparesis. (B) A magnetic resonance imaging time-of-flight angiogram depicting critical stenosis at the left internal carotid artery bulb (white arrow) with 360° coiled distal internal carotid artery (black arrow).
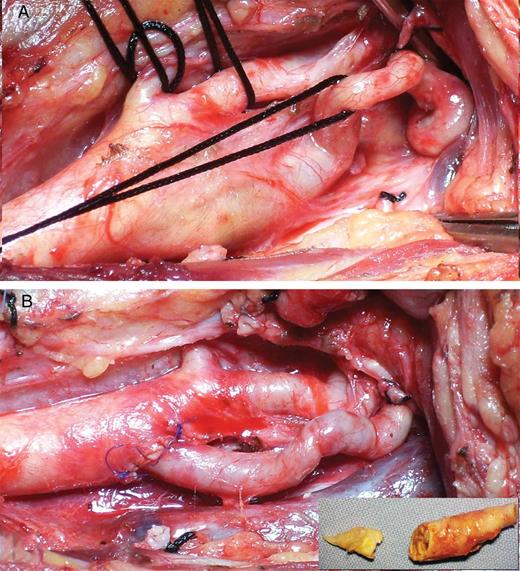
(A) Intraoperative image after dissection of carotid arteries showing plaque-bearing segment of the internal carotid artery bulb, severely coiled and redundant distal internal carotid artery, external carotid artery and superior thyroid artery. Internal carotid artery (ICA) tortuosity from vessel wall weakening can be an aftermath of ageing and atherosclerosis while congenital tortuosity accelerates atherosclerosis by producing flow irregularities. (B) Reimplantation of the straightened and spatulated internal carotid artery onto the carotid bifurcation. Advantages of the ICA ‘resection and reimplantation’ technique include rapid plaque extraction obviating the need to do ICA endarterectomy, decreased susceptibility to restenosis and avoidance of prosthetic patch material. (inset) Resected plaque-bearing segment of internal carotid artery along with endarterectomized common carotid artery plaque. The proximal disease at the common carotid artery (CCA) end was cleared though a sufficient arteriotomy prior to reimplantation of healthy distal ICA onto the CCA.

{kind=link}