






Abstract
We report a patient with Takayasu's disease surgically treated who had presented severe manifestation due to aortic coarctation associated with occlusion of all arch branches. This patient had suffered cardiac failure and recurrent fainting attacks before surgery. The operative procedures included ascending to infra-renal aortic bypass grafting combined with reconstruction of the right axillary artery. Cardio-pulmonary bypass (CPB) was used to facilitate the proximal aortic anastomosis. Regional oxygen saturation in the bilateral frontal lobes was measured intraoperatively using near-infrared spectroscopy to detect cerebral ischemia. Regional oxygen saturation was managed above the critical level throughout the CPB. No new cerebral complications occurred in the perioperative period.
1 Introduction
Takayasu's arteritis has been a non-specific inflammatory disease of unknown etiology since its first description in 1908 [1]. Indication for surgical repair in this disease is often severe circulatory complications including uncontrollable hypertension and cardiac failure [2,3]. A number of factors test the ingenuity of the surgeon to design operative procedures and prepare adjunct measures, such as multiple vessel involvement, substantial changes to affected arterial tissue and concomitant critical complications [2].
We experienced a patient affected by this disease who had presented an extremely critical manifestation before surgical correction. The heart had been in danger of being excluded from all essential organs, because of the existence of severe coarctation in the proximal descending aorta associated with occlusion of all arch branches. We present the multimodal strategy which consisted of designing bypass procedures, using of circulatory assistance to facilitate aortic anastomosis and applying intraoperative detection of brain ischemia.
2 Case report
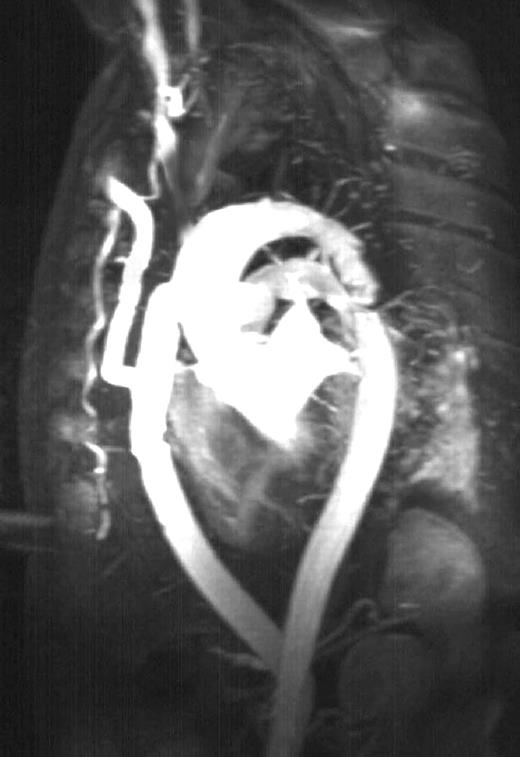
A 61 year-old male was admitted to our hospital with acute cardiac failure. He had a 30-year history of hypertension, and had left hemiparesis resulting from previous cerebral infarction. The result of physical examination showed the absence of a brachial and radial pulse in both upper limbs. The blood pressure in the lower limbs was 82/50 mmHg. Transesophageal echography demonstrated both left ventricular hypertrophy and coarctation in the proximal descending aorta. Magnetic resonance imaging (MRI) showed an aortic lesion associated with occlusion of all arch branches (Fig. 1) . The right subclavian artery was visualized, whereas the left was not. The diagnosis of Takayasu's arteritis was confirmed. The cerebral circulation was supplied by the bilateral vertebral arteries which were perfused via collateral vessels. The patient experienced faintness attacks frequently before surgery.

Preoperative magnetic resonance aortography demonstrates atypical coarctation in the proximal descending aorta. All arch branches are occluded. Collateral vessels to the vertebral arteries originate in the descending aorta.
Surgical treatment was given 3 months after admission. During the operation, the regional oxygen saturation (rSO2) was continuously measured by near-infrared spectroscopy (NIRS) to detect cerebral ischemia using TOS-96 (TOSTEC, Tokyo, Japan). The TOS probe was attached on the midforehead. The blood pressure gradient through the coarctation was found to be 80 mmHg in an intraoperative study. A 16 mm tube graft was anastomosed to the infrarenal aorta and a 8 mm PTFE graft was anastomosed to the right axillary artery. When a partial clamp was placed on the ascending aorta for testing, the blood pressure there rose from 160 to 250 mm Hg. Therefore, we decided to use cardio-pulmonary bypass (CPB) to reduce blood pressure during aortic clamping. To establish CPB circulation, the abdominal aorta and the right axillary artery were simultaneously perfused through tube grafts. Proximal aortic anastomosis was performed using another 16 mm tube, and the suture site was reinforced with a felt strip. The value of rSO2 decreased on initiating circulatory assistance, and it was maintained above 60% throughout CPB with a pump flow rate at 2.3 l/min. After discontinuing CPB, aortic bypass was completed by anastomosing the aortic grafts. Finally, the axillary artery was reconstructed by connecting the 8 mm graft to the aortic graft.
The present patient had no new cerebral complications postoperatively. The systolic blood pressures of the right upper limb and the lower limb were equal at 144 mmHg. The symptoms of cardiac failure and fainting attacks disappeared. An MRI demonstrated the patency of all grafts (Fig. 2) .
Postoperative magnetic resonance aortography demonstrates the patency of the aortic and axillary grafts.
3 Discussion
Aortic bypass has been generally selected for the surgical treatment of aortic coarctation in Takayasu's arteritis, because it can minimize manipulation of the affected aorta. Before the present intervention, we had estimated that excessive blood pressure would disrupt clamping of the ascending aorta for proximal suturing. Therefore, CPB equipment was prepared and standing by. The NIRS equipment was also prepared, because cerebral ischemia could easily occur during CPB. We had intended to manage CPB by perfusing the abdominal aorta and the right axillary artery. Suturing was completed before proximal aortic anastomosis. The use of CPB may be controversial for such patients, in view of the risk of ischemic brain injury. However, a deterioration of hemodynamics at test clamping necessitated circulatory assistance in this patient.
Although arch vessel involvement is a common complication in this disease, a surgical case with occlusion of all arch branches has not been reported previously. Revascularization of all arch vessels was undoubtedly an ideal method to relieve this patient from brain ischemia. However, preoperative studies could not certify the patency of arch branches other than the right subclavian artery, and only reconstruction of that artery was possible.
Near-infrared spectroscopy is a non-invasive optical monitoring technique that provides information on changes in cerebral oxyhemoglobin (oxy-Hb) and deoxyhehomoglobin (deoxy-Hb). This modality has been proposed for intraoperative detection of cerebral ischemia during cardiovascular surgery [4,5]. Regional oxygen saturation in tissue was calculated using an equation: rSO2=oxy-Hb/(oxy-Hb+deoxy-Hb). We estimate the rSO2 value predicting brain ischemia to be less than 60%, because the normal range of rSO2 is calculated to be 60–70% using the normal values of arterial and venous oxygen saturation. While rSO2 once decreased and then recovered during clamping of the axillary artery and CPB in this patient, it was maintained above the critical level during these procedures. NIRS monitoring was helpful to determine an adequate rate of pump flow to both reduce aortic pressure and prevent brain ischemia during CPB.

{kind=link}
{kind=link}