






Abstract
Objectives: There has been no method which can measure regional myocardial blood flow in real-time and continuously. The purpose of this study was to validate myocardial blood flow measurement using a thermal diffusion method. For this purpose, myocardial blood flow measurement was performed using the thermal diffusion method and the electrolytic hydrogen clearance method. Methods: Seven pigs were used for this study, six were for comparison between the thermal diffusion and electrolytic hydrogen clearance methods, and one was for demonstration of myocardial blood flow measurement using the thermal diffusion method on a beating heart coronary artery bypass model with ischemic preconditioning. Results: A good correlation was found between myocardial blood flow values obtained by the electrolytic hydrogen clearance method and 1/V values obtained by a thermal diffusion probe, the correlation coefficient was 0.841 (P≪0.001). During the beating heart coronary artery bypass, the regional myocardial blood flow was recorded in real-time and continuously. Conclusions: This study demonstrated measurement of regional myocardial blood flow using the thermal diffusion method for the first time and simultaneous measurement using the electrolytic hydrogen clearance method for calibration. It provided a real-time and continuous myocardial blood flow measurement and has a potential to contribute to progress in beating-heart surgery.
1 Introduction
During the past decade, major progress has been made in the evolution of technology directed toward the accurate measurement of regional myocardial blood flow (MBF) [1]. However, there has been no method which can measure regional MBF in real-time and continuously. Old fashioned methods, such as the gas clearance method including the electrolytic hydrogen clearance made it possible to measure regional MBF, but real-time monitoring cannot be performed with these methods [1–3]. Widespread modern techniques, including positron emission tomography and magnetic resonance imaging can measure not only regional, but also global MBF; however, these techniques cannot also provide real-time and continuous MBF information [4,5]. Myocardial contrast echocardiography can provide regional real-time MBF information, but continuous monitoring cannot be performed with it because of the temporality of the contrast agent [6].
Real-time continuous tissue blood flow measurement has been made possible in other organs such as the liver and the brain using laser-Doppler perfusion imaging and the thermal diffusion method [7–10]. It is thought that the laser-Doppler perfusion imaging method cannot be applied to MBF measurement because it is theoretically impossible to accurately assess the laser-Doppler effect under heart beating conditions. However, the thermal diffusion method is independent of the subject's motion, and only close connection of a subject to thermal diffusion probe is required. Thus, the thermal diffusion method can potentially be applied to MBF measurement.
The purpose of this study was to validate MBF measurement using the thermal diffusion method. For this purpose, MBF measurement was performed using a thermal diffusion probe, and the electrolytic hydrogen clearance method [2,3], in a stable condition at the same time. Furthermore, demonstration of MBF measurement using the thermal diffusion probe was performed on a beating heart coronary artery bypass model.
2 Material and methods
2.1 The thermal diffusion method
This method is based on the linear relationship between blood flow and the heat conductivity increment in tissue [7–9]. The thermal probe (BTG-221, Biomedical Science Co. Ltd., Kanazawa, Japan) used in this experiment is an updated version of the one described by Koshu and colleagues in 1987 [9]. The probe covered regional myocardium 12 mm in diameter. It consists of a Peltier stack with gold plates arranged so that the voltage output is proportional to the temperature difference between the plates (Fig. 1) . Activation of the stack creates a temperature gradient between the plates which brackets the ambient heart temperature. Blood flow increments temperature gradients cool the heated plate, warm the cold plate, and cause a decrease in the thermocouple voltage output. Thus, tissue blood flow is theoretically inversely proportional to the thermocouple voltage output, and these two parameters should be presented in a simple linear regression [7].
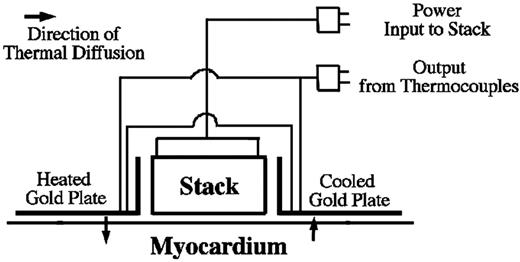
The basic concepts of the thermal diffusion probe.
2.2 The electrolytic hydrogen clearance method
This method is based on the inverse correlation between MBF and hydrogen gas clearance which is electrochemically generated, and the validity of this method for MBF measurement in the beating heart was demonstrated in previous studies [2,3]. For this measurement, an electrolytic hydrogen clearance tissue blood flowmeter (RBF-2, Biomedical Science Co. Ltd., Kanazawa, Japan) was used. The needle electrode is inserted into myocardium and the reference electrode is connected to subcutaneous tissue. A direct current of 50–100 μA is passed for 50 s between the needle electrode and the reference electrode for electrolysis of tissue water. Just after finishing of electrolysis, the electrode changes automatically to monitor the changes in hydrogen concentration by the polarographic current caused by hydrogen oxidation. The half period of the change in hydrogen concentration is calculated and the blood flow is calculated according to a previously described method [2,3].
2.3 MBF measurement using the two methods
Six pigs weighing between 30 and 50 kg were used after ensuring that they were not anemic, their hemoglobin concentration being between 12.0 and 13.0 mg/dl. All animals received human care in compliance with the ‘Principles of Laboratory Animals Care’ formulated by the National Society for Medical Research and the ‘Guide for the Care and Use of Laboratory Animals’ prepared by the Institute of Laboratory Animal Resources and published by the National Institute of Health (NIH Publication No. 86-23, revised 1985).
Anesthesia was induced with an intramuscular administration of ketamine hydrochloride (20 mg/kg). After trachiotomy, a cuffed endotracheal tube was inserted, and ventilation was performed with a volume-regulated ventilator (KMA-1300IIS, Acoma, USA). Then, muscle relaxation was achieved with pancuronium 0.1 mg/kg via peripheral intravenous access. Anesthesia was maintained with 1% halothene. A 4 Fr catheter was inserted into the ascending aorta through the right carotid artery to achieve continuous aortic pressure. Following median sternotomy, the heart was elevated in a pericardial sling. The thermal diffusion probe was sutured on the surface of the heart at the anterior wall of the left ventricle, the needle electrode was inserted approximately 3 mm proximal the probe into the myocardium for preventing interference between the two methods, and the reference electrode was placed in the subcutaneous space (Fig. 2) . Stable MBF values by the thermal diffusion probe could be obtained 30 s after attachment. After stabilization of the recording, measurements were made in parallel using the two methods. Changes in blood flow were made several times by changing the dopamine concentration from 0 to 10 μl/min per kg.
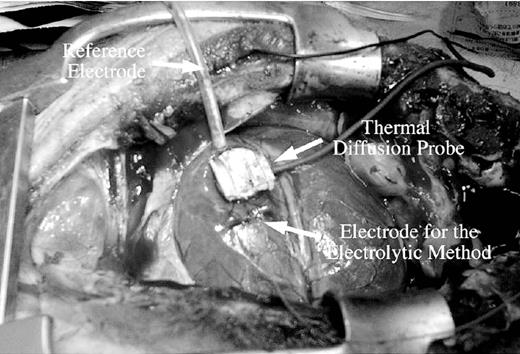
A thermal diffusion probe, an electrode and a reference electrode for the electrolytic hydrogen clearance method are set on the surface of a pig heart. The thermal diffusion probe was sutured on the heart at the anterior wall of the left ventricle at a point 2 cm distal from the first diagonal branch and 1 cm away from the left anterior descending coronary artery.
2.4 Demonstration of MBF measurement with a thermal diffusion probe
A pig weighing 42 kg was used for this experiment. Animal preparation was the same as detailed above. The left intrathoracic artery was dissected for the graft and the thermal diffusion probe was placed on the surface of the heart at the anterior wall of the left ventricle. After administration of 200 U/kg of heparin sodium, ischemic preconditioning with two periods of 5-min coronary occlusion and 5-min reperfusion was performed. Then, a heart stabilizer [11] was attached to the left anterior descending coronary artery and coronary arteriotomy was performed. The anastomosis of the graft to the coronary artery was performed in the usual way. The MBF at the anterior wall of the left ventricle was continuously recorded using a thermal diffusion probe during this procedure.
2.5 Statistical analysis
Simple linear regression was used to analyze the relationship between the MBF obtained by the electrolytic method and the 1/V obtained by the thermal diffusion method.
3 Results
The data obtained by the thermal diffusion and electrolytic methods are plotted in Fig. 3 and linear regression analysis was performed. A good correlation was found between MBF values obtained by the electrolytic hydrogen clearance method and 1/V values obtained by the thermal diffusion probe; the correlation coefficient was 0.841 (P≪0.001).
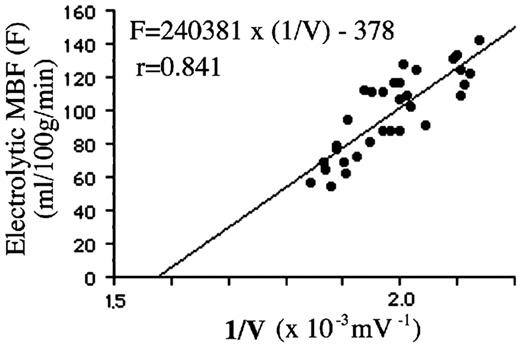
Correlation between myocardial blood flow (MBF) obtained by the electrolytic hydrogen clearance method and the 1/V value obtained by the thermal diffusion probe.
The demonstration of MBF measurement using the thermal diffusion probe is shown in Fig. 4 . MBF was continuously recorded in real-time, and regional MBF immediately decreased after occlusion and increased after reperfusion of the coronary artery.

Demonstration of myocardial blood flow (MBF) measurement. In this experiment, the thermal diffusion probe presented relatively little decrease during total left anterior descending coronary artery occlusion. This result may be due to the blood flow from the diagonal branch near to the probe (Fig. 2).
4 Discussion
In this study, regional MBF was measured in real-time and continuously for the first time to our knowledge using the thermal diffusion method. MBF measured with the electrolytic hydrogen clearance method significantly correlated with 1/V values obtained by the thermal diffusion probe. This means that MBF can be measured using the thermal diffusion method continuously, and the value was reliable similar to that measured by the electrolytic hydrogen clearance method.
The thermal diffusion method has been investigated and improved for a long time. At first, it was developed mainly in the field of neurosurgery. In 1968, Brawley reported that the Peltier stack commonly used in electric refrigerators could be used in the thermal diffusion method [12], and marked improvements in the stability of recordings using this method were thereby obtained. Subsequently, Carter and colleagues made improvements in the probe itself and associated equipment [8]. On the basis of their experimental findings, they devised a means for quantifying blood flow and put their method to practical use. Nowadays, it has been applied for many organs, including the liver [10], the kidney [13], and peripheral extremities [14]. However, it has not been applied to the myocardium and this study is the first report on the thermal diffusion method applied for MBF measurement.
MBF measurement using the thermal diffusion method has great potentials for both experimental investigations and clinical cardiac surgery. It requires no special equipment or environment, unlike positron emission tomography, magnetic resonance imaging, or X-ray machines, and it can be used anywhere. Moreover, MBF measurement using the thermal diffusion method can be performed continuously during heart manipulation. Considering such convenient and continuous features, the thermal diffusion method can contribute particularly to progress in beating-heart surgery. Although several methods were suggested for myocardial protection during beating-heart coronary artery bypass surgery [15–17], there has been no study to investigate the validity of the protective effect in terms of continuous myocardial blood flow. Experimental verification of myocardial protective procedures for the beating-heart with the thermal diffusion method could decide a superior procedure; moreover, a novel innovative procedure may be devised.
On the other hand, there are several points to be improved and studied in future investigations. In the present study, the thermal diffusion probe was sutured on the left ventricle, and it may change regional MBF itself and affect adversely to the myocardium. Thus, this probe cannot apply for clinical settings as it was. However, we are now devising a method which attaches the probe to the myocardium with a suction system, and if these problems will be solved the thermal diffusion method can provide useful information to surgeons performing clinical beating-heart surgery. At present, myocardial ischemia can be roughly assessed mainly from changes in electrocardiogram changes, homodynamic conditions, and myocardial wall motion detected by transesophageal echocardiography [18]. MBF can be estimated using transit-time coronary blood flow measurement, but this information can be obtained only through a graft and it can not treat problems during anastomosis in beating-heart surgery [19,20]. Thermal coronary angiography using near-infrared camera systems can assess regional MBF very roughly, however this method can provide neither continuous or quantitative information [21,22]. The thermal diffusion method can provide accurate evaluation of regional MBF and it will contribute to an improvement in the safety of beating-heart surgery.
In conclusion, this study demonstrated measurement of MBF with the thermal diffusion method for the first time, with simultaneous measurement with the electrolytic hydrogen clearance method for calibration. It provided a real-time and continuous MBF measurement and has a potential to contribute to progress in beating-heart surgery.

{kind=link}
{kind=link}
{kind=link}
{kind=link}