





Abstract
The impact of the COVID-19 pandemic on multimodal cardiac rehabilitation (CR) programmes has forced a continuous readjustment of clinical practice. Our regional healthcare system was faced with providing quality remote CR to ischaemic heart disease (IHD) patients in a scattered, mostly rural population, for which three new CR modalities replaced the previous in-person CR program: 1) telephone follow-up programme, 2) TELEA online platform for patient follow-up and 3) TELEA online follow-up & online training sessions.
To study the impact of the COVID-19 pandemic on CR offering and acceptance and the reasons for patient refusal, and to assess the outcome of new remote CR modalities in this setting.
Single center, observational retrospective study from all consecutive patients with IHD eligible for CR from 2015 to 2021. A descriptive analysis of patient baseline characteristics, CR modality, offering and acceptance rates, and reasons for refusal per year was performed. Additionally, a comparative analysis of “pre-COVID period” (Jan 2015–Feb 2020) vs. “COVID period” (Mar 2020–Dec 2021) was performed to assess the impact of the pandemic on patient recruitment and the usefulness of remote CR modalities to enhance participation.
N=2626 patients (20% women, 69.7±45.8 years) were offered CR from 2015 to 2021. CR offering decreased from the pre-COVID (78.6%) to the COVID period (52.6%), while participation increased (67.9% and 79.7%, respectively) Figure 1. Reasons for CR refusal significantly changed with an odds ratio (OR) of 5.63 and confidence interval (CI) 95% (3.2–9.9). In the pre-COVID period main reasons for CR refusal was “transportation difficulties” (47%); while during the COVID-19 period, the main reason shifted to “lack of interest” (78.2%) (Table 1).
Offering CR decreased during the COVID pandemic possibly due to stricter inclusion criteria. However, the implementation of new remote CR modalities allowed not only to maintain similar levels of acceptance but also to improve it despite the unfavourable setting, and helped to amend transportation difficulties as the leading reason for refusal. Remote CR may be a useful tool, combined with in-person programs, to enhance participation in CR.
Type of funding sources: None.
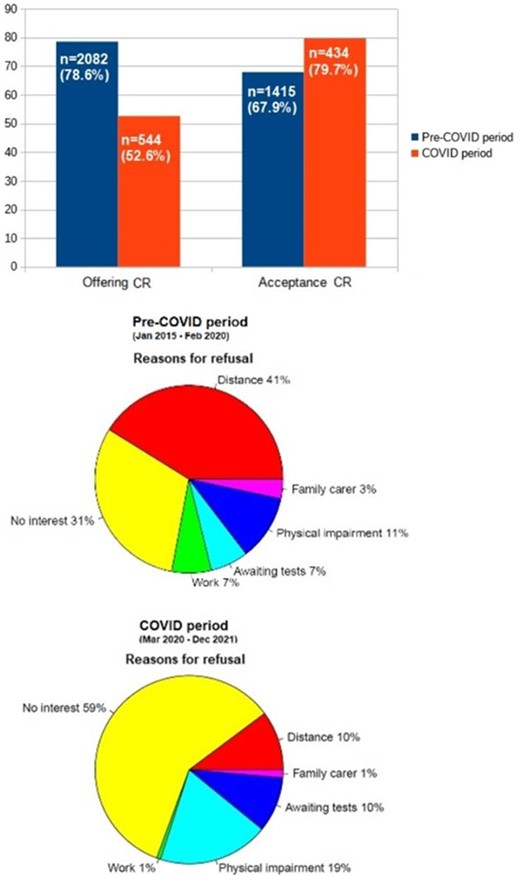
Figure 1


{kind=link}