




Abstract
Transcatheter aortic valve replacement-related infective endocarditis (TAVR-IE) is associated with a poor prognosis. TAVR-IE diagnosis is challenging, and benefits of the most recent classifications [European Society of Cardiology (ESC)-2015, International Society for Cardiovascular Infectious Diseases (ISCVID)-2023, and ESC-2023] have not been compared with the conventional Duke criteria on this population. The primary objective was to compare the diagnostic value of the Duke, ESC-2015, ISCVID-2023, and ESC-2023 criteria for the diagnosis of TAVR-IE. The secondary objectives were to determine which criteria increase the diagnostic accuracy of each classification and to evaluate in-hospital and 1-year mortality of TAVR-IE.
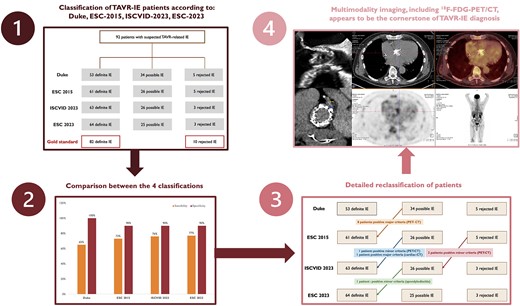
From January 2015 to May 2022, 92 patients with suspected TAVR-IE were retrospectively included in two French centres, including 82 patients with definite TAVR-IE and 10 patients with rejected TAVR-IE as defined by expert consensus. Duke classification yielded a sensitivity of 65% [95% confidence interval (CI): 53–75%] and a specificity of 100% (95% CI: 69–100%) for the diagnosis of TAVR-IE. ESC-2015 classification increased Duke criterion sensitivity from 65 to 73% (P = 0.016) but decreased specificity from 100 to 90%. ISCVID-2023 and ESC-2023 also increased Duke criterion sensitivity from 65 to 76% (P = 0.004) and 77% (P = 0.002), respectively, but also decreased specificity from 100 to 90%. A positive 18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) was the most helpful criterion, as 10 patients (11%) were correctly reclassified. In-hospital mortality after TAVR-IE was 21% and 1-year mortality was 38%.
A multimodality imaging approach, including 18F-FDG PET/CT and gated cardiac CT, is the cornerstone of TAVR-IE diagnosis and explains the higher sensitivity of ESC-2015 and recent classifications compared with Duke criteria.



{kind=link}