





Abstract
Type of funding sources: None.
Transcatheter edge-to-edge tricuspid valve repair (TTVR) for tricuspid regurgitation (TR) is an emerging treatment option in inoperable patients. TTVR is always guided by transesophageal echocardiography (TOE) and performed under general anesthesia. In patients with excellent acoustic window, transthoracic echocardiography (TTE) can also provide a comprehensive morphological understanding. Moreover, in TTVR there is no need for transseptal puncture.
We investigated if TTVR can be successfully conducted by a novel TTE guiding approach, in conjunction with fluoroscopy, based on the concept of the 4 right-sided chamber views.
Thirty TTVR patients were assigned to a TTE (n=10) and a TOE group (n=20), depending on acoustic window and corresponding guidance. Multimodality imaging was paramount for procedural planning and included TTE, TOE and cardiac CT, from which the corresponding fluoroscopic angulations of the 4 right-sided chamber views were derived. Thus, interventionalists and cardiac imaging specialists were assessing the same chamber views from their respective imaging modality. TR severity and quality of life parameters were assessed at baseline and up to 12 months.
Except for lower BMI (TTE 22.3±0.8 vs TOE 29.8±4.3, p<0.001), baseline characteristics were similar between groups e.g., age (81.7±3.9 vs 82.8±4.1, p = 0.483) or EuroSCORE II (11.9±10.3 vs 10.4±8, p = 0.692). Device success was achieved in all patients, with a total of 15 implanted clips in the TTE (clips / patient 1.5±0.7) vs 31 clips in the TOE group (1.5±0.6), and device times of 75±37.1 vs 65.7±31.3 minutes (p = 0.506). TR reduction was successful in all but one patient, in each group (90% vs 95%, p = 1.000). TR improvement was equal between-groups, with 2- or more grade reduction in 60% of cases, at 30 days. No device associated complications occurred.
Nine patients in the TTE group and 17 in the TOE group completed one-year follow-up. Quality of life and functional capacity similarly improved in both groups, with NYHA class reduction in all survivals [100% (9/9) vs 95% (17/17), p = 1.000], and significant improvement in KCCQ score and 6-minute walk distance in each respective group (∆24.8±21.4 vs 20.1±13.6 points, p = 0.227; ∆93.5±100.4 vs 80.8±64 meters, p = 0.121). TR reduction impacted major organs e.g., liver and kidney. Thus, glomerular filtration rate (GFR) increased [TTE group 56.8±18.7 vs 64.6±14.9 ml/m2/1,73m2, p = 0.050; TOE group 50.7±19.9 vs 53.8±20.9, p = 0.347], while liver congestion parameters decreased e.g, aspartate aminotransferase (AST) [TTE group 28.6±7.5 vs 26.2±8.6 U/L, p = 0.274; TOE group 33.1±5.8 vs 23.6±9, p = 0.388].
TTE guidance of TTVR is feasible in selected patients with excellent acoustic window and represents an alternative to TOE or, in combination, may facilitate transition to conscious sedation. Successful TTVR leads to improvement in quality of life, symptom control, and multiorgan function.
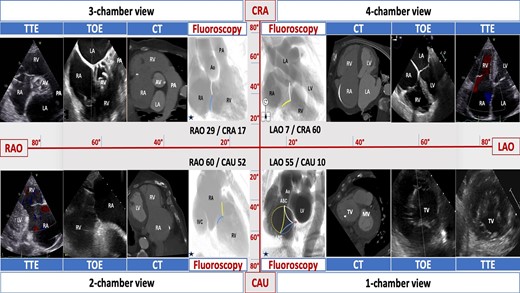
The 4 right-sided chamber views
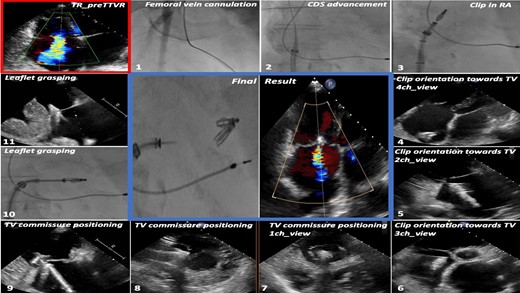
Methodology of TTE guidance of TTVR

{kind=link}