





Abstract
Echocardiography is less than 70 years old, and many major advances have occurred within living memory, but already some pioneering contributions may be overlooked. In order to consider what circumstances have been common to the most successful innovations, we have studied and here provide a timeline and summary of the most important developments in transthoracic and transoesophageal ultrasound imaging and Doppler techniques, as well as in intravascular ultrasound and imaging in paediatric cardiology. The entries are linked to a comprehensive list of first publications and to a collection of first-hand historical accounts published by early investigators. Review of the original manuscripts highlights that it is difficult to establish unequivocal precedence for many new imaging methods, since engineers were often working independently but simultaneously on similar problems. Many individuals who are prominently linked with particular developments were not the first in their field. Developments in echocardiography have been highly dependent on technological advances, and most likely to be successful when engineers and clinicians were able to collaborate with open exchange between centres and disciplines. As with many other new medical technologies, initial responses were sceptical and introduction into clinical practice required persistence and substantial energy from the first adopters. Current developments involve advances in software as much as in equipment, and progress will depend on continuing collaborations between engineers and clinical scientists, for example to identify unmet needs and to investigate the clinical impact of particular imaging approaches.
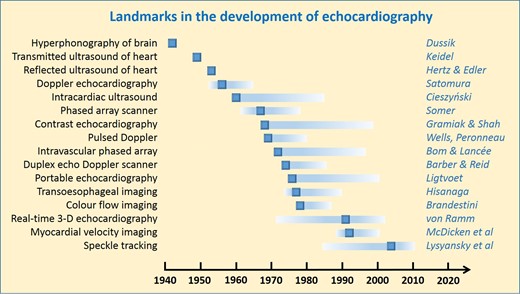
Selected principal milestones in the development of echocardiography. Details and references can be found in the text, timeline, and references.
Introduction
Ultrasound imaging is the only major medical imaging modality for which no-one was awarded a Nobel Prize. Although some investigators were nominated, notably Edler and Hertz as pioneers of cardiac imaging, it may have been difficult for the nominating committee to establish precedence since the development of ultrasound for cardiovascular imaging depended on many prior insights from physics (Figure 1), initial technical developments, and preliminary clinical experiments. Nonetheless, certain major milestones can be identified.
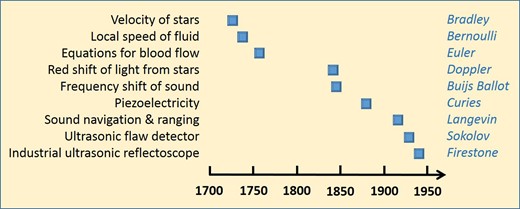
Timeline of key insights from physics that remain important for current echocardiographic practice.
Echocardiography is now an ubiquitous and essential diagnostic investigation, yet the first exploratory studies were performed less than 70 years ago, and the technique became established in clinical practice only about 50 years ago. Many key advances are still within living memory. To understand why and how early experiments were performed and prototypes were developed, we identified and have reviewed the original publications, as well as first-hand accounts of their research published or described by pioneering investigators. We provide a timeline of the most important developments, cross-referenced to the first or key publications1–94 (Table 1). The objective of this historical perspective is to provide an authoritative summary in a single publication, from which we can identify common circumstances that may contribute to successful innovation and implementation of effective new diagnostic methods
Cardiac and cardiovascular ultrasound timeline
| Year | Scientific contribution |
|---|---|
| 1727 | James Bradley reported the aberration of light from stars, and measured its speed.1 |
| 1738 | Daniel Bernoulli related the speed of a fluid to a local decrease in pressure or potential energy.2 |
| 1757 | Leonhard Euler (who had studied with Bernoulli’s father) published general principles of fluid dynamics,3 followed in 1775 by his publication on flow in blood that is still applicable to non-invasive haemodynamic assessments.4 |
| 1842 | Christian Doppler gave paper ‘On the coloured light of the double stars and certain other heavenly bodies’5 to the Royal Bohemian Society of Sciences, Prague, 25th May (which was a theoretical development of the earlier paper by James Bradley). |
| 1845 | Christophorus Hendrik Diederik Buijs Ballot, observed the frequency shift of sound waves.6 |
| 1880 | Jacques and Pierre Curie discovered the piezoelectric effect.7 |
| 1916 | Paul Langevin (who had been a doctoral student of Pierre Curie) developed SONAR during the First World War; he filed patents with Constantin Chilowsky in 1916 in France8 and 1917 in the USA9 (stating that ‘The relative motion of the obstacle and the observation post may be determined by applying Doppler’s method..’). |
| 1929 | Sokolov in Russia proposed using ultrasound to test castings.10 He filed a US patent application for his ultrasonic flaw detector (as Sergey Sokoloff) in 1937.11 |
| 1940 | Floyd Firestone constructed an ultrasonic reflectoscope for industrial use.12 He applied for a patent during the Second World War, and published his method afterwards in 1946.13 |
| 1942 | Karl Theo Dussik developed what he called ‘hyperphonography’, using transmitted US to examine the brain,14,15 he considered but did not pursue ultrasound reflection. |
| 1949 | Wolf-Dieter Keidel scanned the heart with transmitted ultrasound, to estimate its volume (after trying but rejecting the pulse-reflection method).16,17 |
| 1952 | John Wild and John Reid applied echo-ranging to determine the structure of biological soft tissues (including breast).18–20 Figures include ‘A-mode’ demonstration. (John Wild started his research after locating to the USA in 1946). |
| 1952 | Douglass Howry & Roderic Bliss produced compound scans of human anatomy, equivalent cumulatively to 2D cross-sections (‘Somascope’),21,22 first results obtained in 1950. |
| 1953 | May: first trial by Hellmuth Hertz and Inge Edler on themselves of ultrasound using machine from Kockum shipyard; first A-mode scan (reflected ultrasound) of heart. |
| 1953 | 29th October, first M-mode scan by Edler and Hertz. Published 1954.23 |
| 1955 | Ian Donald (who met John Wild in London in the early 1950 s) starts to investigate reflected ultrasound in the abdomen and then in obstetric practice, like Edler and Hertz starting with a borrowed flaw detector; with engineer Tom Brown, develops ‘Diasonograph’ which produced compound obstetric scans.24 |
| 1956 | Shigeo Satomura, ultrasonic Doppler method to measure cardiac motion (with continuous wave). Initial report in Japanese,25 first publication in English in 1957.26 |
| 1960 | Tomasz Cieszyński, first intravascular scanning and intracardiac echocardiography reported, using a single-element transducer on a catheter (developed from 1956).27 |
| 1961 | Edler’s thesis published as supplement to Acta Medica Scandinavica.28 |
| 1962 | Ryozo Omoto obtained 2D intravascular images with a slowly rotating, single-element transducer mounted at a catheter tip.29,30 First publication in English in 1967.31,32 |
| 1963 | First dedicated cardiac ultrasound scanner built by John (Jack) Reid, working with cardiologist Claude Joyner.33 |
| 1963 | Olofsson develops an optical mirror system for 2D scanning of the heart,34 working with Hertz.35 Further development reported by Arne Åsberg (1967).36 |
| 1964 | ‘Ultrasono-cardio-tomography’ reported from Sendai, Japan, for 2D imaging using mechanical sector scanning.37–39 |
| 1967 | Francis McLeod, directional Doppler system.40 |
| 1967 | Jan Somer constructed first electronic phased-array scanner (‘Electroscan’).41,42 |
| 1968 | Raymond Gramiak and Pravin Shah, first report of (M-mode) contrast echocardiography.43 |
| 1968 | Daniel Kalmanson, directional flow measurement by continuous wave Doppler.44 |
| 1969 | Range-gated (pulsed) Doppler ultrasound developed by three groups: in 1969 Peter Wells45 (Bristol) and Paul Peronneau46 (Paris); and then Donald Baker47 (1970). |
| 1969 | Transthoracic (continuous wave) recording of aortic flow by Henry Light.48 |
| 1971 | Nicolaas (Klaas) Bom and Charles Lancée, first real-time 2D (linear array) cardiac scans (‘Multiscan’).49,50 |
| 1972 | Bom and colleagues, first catheter-based cylindrical phased-array ultrasonic intravascular/intracardiac transducer.51 |
| 1972 | First textbook on echocardiography (Harvey Feigenbaum).52 |
| 1973 | First clinical reports on 2D echo (using the Multiscan) by Frank Kloster53 and Jos Roelandt,54 with Bom and colleagues. |
| 1973 | James Griffith and Walter Henry, mechanical sector scanner for 2D imaging.55,56 |
| 1974 | Frederick Thurstone and Olaf von Ramm, phased-array scanner,57,58 clinical studies reported by Joe Kisslo.59 |
| 1974 | Frank Barber with John Reid, ultrasonic duplex echo-Doppler scanner.60 |
| 1974 | Prototype for 3D cardiac imaging by combining 2D images acquired in different planes (Dekker et al.).61 |
| 1974 | Louis Teichholz publishes method for calculating ejection fraction from left ventricular echocardiographic dimensions.62 |
| 1974 | Bjørn Angelsen constructed a pulsed Doppler system for recording aortic blood flow.63 |
| 1976 | Lee Frazin, single-element transoesophageal echocardiography.64 |
| 1976 | Jarle Holen, first publication using Doppler ultrasound to estimate pressure gradients in heart valve disease (using a modified Gorlin formula).65 |
| 1976 | Cees Ligtvoet with N Bom and colleagues in Rotterdam, first portable (‘hand-held’) echocardiography system (‘Minivisor’),66 clinical study published in 1978.67 |
| 1977 | Kohzoh Hisanaga, high-speed rotating cross-sectional transoesophageal scanner.68,69 |
| 1977 | Alf Brubakk with Bjørn Angelsen and Liv Hatle proposed a modified Bernoulli equation for Doppler echocardiography to assess the severity of heart valve disease.70 |
| 1978 | Marco Brandestini, multigated Doppler instrument, combining imaging of flow encoded in colour, superimposed initially on M-mode scans and later on 2D images.71–73 |
| 1978 | Griffith and Henry, combined instrument for imaging and Doppler.74 |
| 1978 | Hatle with Angelsen, quantification of mitral stenosis75 (1978) and aortic stenosis76 (1980) by the modified Bernoulli method. |
| 1979 | First report of exercise stress echocardiography using 2-dimensional imaging by Wann et al.,77 further developed by Morganroth,78 and Maurer,79 in 1981. |
| 1981 | Jacques Souquet, Peter Hanrath, transoesophageal phased-array echocardiography.80,81 |
| 1982 | First textbook on Doppler Echocardiography (Bjørn Angelsen and Liv Hatle).82 |
| 1982 | Chihiro Kasai,83 with Koroku Namekawa et al.: first commercial real-time colour flow imaging system, using autocorrelation, from Aloka; initial clinical publication by Ryozo Omoto.84 |
| 1982 | Pulsed Doppler recording of mitral flow proposed by Akira Kitabatake for the assessment of left ventricular diastolic function.85 |
| 1983 | First commercial system with colour flow mapping (Aloka). |
| 1989 | Karl Isaaz, proof of concept for regional myocardial velocity measurement.86 |
| 1991 | Olaf von Ramm, first real-time 3D imaging system (‘Volumetrics’).87 |
| 1992 | Multiplane transoesophageal echocardiography (Hewlett Packard).88 |
| 1992 | Norman McDicken and George Sutherland, development of colour and pulsed tissue Doppler (with Acuson).89 |
| 1998 | Software for imaging of regional myocardial function based on post-processing of colour tissue Doppler, by Lars-Åke Brodin and Bjørn Olstad.90 |
| 1998 | Myocardial strain rate, developed by Andreas Heimdal et al.91 |
| 2004 | Peter Lysyansky et al., first commercial system for speckle tracking of grey-scale images, leading to measurement of global longitudinal strain.92,93 |
| 2008 | Real-time ‘live’ 3D transoesophageal imaging (Lissa Sugeng et al.).94 |
| Year | Scientific contribution |
|---|---|
| 1727 | James Bradley reported the aberration of light from stars, and measured its speed.1 |
| 1738 | Daniel Bernoulli related the speed of a fluid to a local decrease in pressure or potential energy.2 |
| 1757 | Leonhard Euler (who had studied with Bernoulli’s father) published general principles of fluid dynamics,3 followed in 1775 by his publication on flow in blood that is still applicable to non-invasive haemodynamic assessments.4 |
| 1842 | Christian Doppler gave paper ‘On the coloured light of the double stars and certain other heavenly bodies’5 to the Royal Bohemian Society of Sciences, Prague, 25th May (which was a theoretical development of the earlier paper by James Bradley). |
| 1845 | Christophorus Hendrik Diederik Buijs Ballot, observed the frequency shift of sound waves.6 |
| 1880 | Jacques and Pierre Curie discovered the piezoelectric effect.7 |
| 1916 | Paul Langevin (who had been a doctoral student of Pierre Curie) developed SONAR during the First World War; he filed patents with Constantin Chilowsky in 1916 in France8 and 1917 in the USA9 (stating that ‘The relative motion of the obstacle and the observation post may be determined by applying Doppler’s method..’). |
| 1929 | Sokolov in Russia proposed using ultrasound to test castings.10 He filed a US patent application for his ultrasonic flaw detector (as Sergey Sokoloff) in 1937.11 |
| 1940 | Floyd Firestone constructed an ultrasonic reflectoscope for industrial use.12 He applied for a patent during the Second World War, and published his method afterwards in 1946.13 |
| 1942 | Karl Theo Dussik developed what he called ‘hyperphonography’, using transmitted US to examine the brain,14,15 he considered but did not pursue ultrasound reflection. |
| 1949 | Wolf-Dieter Keidel scanned the heart with transmitted ultrasound, to estimate its volume (after trying but rejecting the pulse-reflection method).16,17 |
| 1952 | John Wild and John Reid applied echo-ranging to determine the structure of biological soft tissues (including breast).18–20 Figures include ‘A-mode’ demonstration. (John Wild started his research after locating to the USA in 1946). |
| 1952 | Douglass Howry & Roderic Bliss produced compound scans of human anatomy, equivalent cumulatively to 2D cross-sections (‘Somascope’),21,22 first results obtained in 1950. |
| 1953 | May: first trial by Hellmuth Hertz and Inge Edler on themselves of ultrasound using machine from Kockum shipyard; first A-mode scan (reflected ultrasound) of heart. |
| 1953 | 29th October, first M-mode scan by Edler and Hertz. Published 1954.23 |
| 1955 | Ian Donald (who met John Wild in London in the early 1950 s) starts to investigate reflected ultrasound in the abdomen and then in obstetric practice, like Edler and Hertz starting with a borrowed flaw detector; with engineer Tom Brown, develops ‘Diasonograph’ which produced compound obstetric scans.24 |
| 1956 | Shigeo Satomura, ultrasonic Doppler method to measure cardiac motion (with continuous wave). Initial report in Japanese,25 first publication in English in 1957.26 |
| 1960 | Tomasz Cieszyński, first intravascular scanning and intracardiac echocardiography reported, using a single-element transducer on a catheter (developed from 1956).27 |
| 1961 | Edler’s thesis published as supplement to Acta Medica Scandinavica.28 |
| 1962 | Ryozo Omoto obtained 2D intravascular images with a slowly rotating, single-element transducer mounted at a catheter tip.29,30 First publication in English in 1967.31,32 |
| 1963 | First dedicated cardiac ultrasound scanner built by John (Jack) Reid, working with cardiologist Claude Joyner.33 |
| 1963 | Olofsson develops an optical mirror system for 2D scanning of the heart,34 working with Hertz.35 Further development reported by Arne Åsberg (1967).36 |
| 1964 | ‘Ultrasono-cardio-tomography’ reported from Sendai, Japan, for 2D imaging using mechanical sector scanning.37–39 |
| 1967 | Francis McLeod, directional Doppler system.40 |
| 1967 | Jan Somer constructed first electronic phased-array scanner (‘Electroscan’).41,42 |
| 1968 | Raymond Gramiak and Pravin Shah, first report of (M-mode) contrast echocardiography.43 |
| 1968 | Daniel Kalmanson, directional flow measurement by continuous wave Doppler.44 |
| 1969 | Range-gated (pulsed) Doppler ultrasound developed by three groups: in 1969 Peter Wells45 (Bristol) and Paul Peronneau46 (Paris); and then Donald Baker47 (1970). |
| 1969 | Transthoracic (continuous wave) recording of aortic flow by Henry Light.48 |
| 1971 | Nicolaas (Klaas) Bom and Charles Lancée, first real-time 2D (linear array) cardiac scans (‘Multiscan’).49,50 |
| 1972 | Bom and colleagues, first catheter-based cylindrical phased-array ultrasonic intravascular/intracardiac transducer.51 |
| 1972 | First textbook on echocardiography (Harvey Feigenbaum).52 |
| 1973 | First clinical reports on 2D echo (using the Multiscan) by Frank Kloster53 and Jos Roelandt,54 with Bom and colleagues. |
| 1973 | James Griffith and Walter Henry, mechanical sector scanner for 2D imaging.55,56 |
| 1974 | Frederick Thurstone and Olaf von Ramm, phased-array scanner,57,58 clinical studies reported by Joe Kisslo.59 |
| 1974 | Frank Barber with John Reid, ultrasonic duplex echo-Doppler scanner.60 |
| 1974 | Prototype for 3D cardiac imaging by combining 2D images acquired in different planes (Dekker et al.).61 |
| 1974 | Louis Teichholz publishes method for calculating ejection fraction from left ventricular echocardiographic dimensions.62 |
| 1974 | Bjørn Angelsen constructed a pulsed Doppler system for recording aortic blood flow.63 |
| 1976 | Lee Frazin, single-element transoesophageal echocardiography.64 |
| 1976 | Jarle Holen, first publication using Doppler ultrasound to estimate pressure gradients in heart valve disease (using a modified Gorlin formula).65 |
| 1976 | Cees Ligtvoet with N Bom and colleagues in Rotterdam, first portable (‘hand-held’) echocardiography system (‘Minivisor’),66 clinical study published in 1978.67 |
| 1977 | Kohzoh Hisanaga, high-speed rotating cross-sectional transoesophageal scanner.68,69 |
| 1977 | Alf Brubakk with Bjørn Angelsen and Liv Hatle proposed a modified Bernoulli equation for Doppler echocardiography to assess the severity of heart valve disease.70 |
| 1978 | Marco Brandestini, multigated Doppler instrument, combining imaging of flow encoded in colour, superimposed initially on M-mode scans and later on 2D images.71–73 |
| 1978 | Griffith and Henry, combined instrument for imaging and Doppler.74 |
| 1978 | Hatle with Angelsen, quantification of mitral stenosis75 (1978) and aortic stenosis76 (1980) by the modified Bernoulli method. |
| 1979 | First report of exercise stress echocardiography using 2-dimensional imaging by Wann et al.,77 further developed by Morganroth,78 and Maurer,79 in 1981. |
| 1981 | Jacques Souquet, Peter Hanrath, transoesophageal phased-array echocardiography.80,81 |
| 1982 | First textbook on Doppler Echocardiography (Bjørn Angelsen and Liv Hatle).82 |
| 1982 | Chihiro Kasai,83 with Koroku Namekawa et al.: first commercial real-time colour flow imaging system, using autocorrelation, from Aloka; initial clinical publication by Ryozo Omoto.84 |
| 1982 | Pulsed Doppler recording of mitral flow proposed by Akira Kitabatake for the assessment of left ventricular diastolic function.85 |
| 1983 | First commercial system with colour flow mapping (Aloka). |
| 1989 | Karl Isaaz, proof of concept for regional myocardial velocity measurement.86 |
| 1991 | Olaf von Ramm, first real-time 3D imaging system (‘Volumetrics’).87 |
| 1992 | Multiplane transoesophageal echocardiography (Hewlett Packard).88 |
| 1992 | Norman McDicken and George Sutherland, development of colour and pulsed tissue Doppler (with Acuson).89 |
| 1998 | Software for imaging of regional myocardial function based on post-processing of colour tissue Doppler, by Lars-Åke Brodin and Bjørn Olstad.90 |
| 1998 | Myocardial strain rate, developed by Andreas Heimdal et al.91 |
| 2004 | Peter Lysyansky et al., first commercial system for speckle tracking of grey-scale images, leading to measurement of global longitudinal strain.92,93 |
| 2008 | Real-time ‘live’ 3D transoesophageal imaging (Lissa Sugeng et al.).94 |
Note: the entries in italics concern general or non-cardiac imaging applications.
The dates refer either to the first date of use, if available, or to the earliest publication. The entries relate mostly to engineering and technical developments, rather than to the first reports of new clinical applications or insights. This timeline does not list all early investigators.
Cardiac and cardiovascular ultrasound timeline
| Year | Scientific contribution |
|---|---|
| 1727 | James Bradley reported the aberration of light from stars, and measured its speed.1 |
| 1738 | Daniel Bernoulli related the speed of a fluid to a local decrease in pressure or potential energy.2 |
| 1757 | Leonhard Euler (who had studied with Bernoulli’s father) published general principles of fluid dynamics,3 followed in 1775 by his publication on flow in blood that is still applicable to non-invasive haemodynamic assessments.4 |
| 1842 | Christian Doppler gave paper ‘On the coloured light of the double stars and certain other heavenly bodies’5 to the Royal Bohemian Society of Sciences, Prague, 25th May (which was a theoretical development of the earlier paper by James Bradley). |
| 1845 | Christophorus Hendrik Diederik Buijs Ballot, observed the frequency shift of sound waves.6 |
| 1880 | Jacques and Pierre Curie discovered the piezoelectric effect.7 |
| 1916 | Paul Langevin (who had been a doctoral student of Pierre Curie) developed SONAR during the First World War; he filed patents with Constantin Chilowsky in 1916 in France8 and 1917 in the USA9 (stating that ‘The relative motion of the obstacle and the observation post may be determined by applying Doppler’s method..’). |
| 1929 | Sokolov in Russia proposed using ultrasound to test castings.10 He filed a US patent application for his ultrasonic flaw detector (as Sergey Sokoloff) in 1937.11 |
| 1940 | Floyd Firestone constructed an ultrasonic reflectoscope for industrial use.12 He applied for a patent during the Second World War, and published his method afterwards in 1946.13 |
| 1942 | Karl Theo Dussik developed what he called ‘hyperphonography’, using transmitted US to examine the brain,14,15 he considered but did not pursue ultrasound reflection. |
| 1949 | Wolf-Dieter Keidel scanned the heart with transmitted ultrasound, to estimate its volume (after trying but rejecting the pulse-reflection method).16,17 |
| 1952 | John Wild and John Reid applied echo-ranging to determine the structure of biological soft tissues (including breast).18–20 Figures include ‘A-mode’ demonstration. (John Wild started his research after locating to the USA in 1946). |
| 1952 | Douglass Howry & Roderic Bliss produced compound scans of human anatomy, equivalent cumulatively to 2D cross-sections (‘Somascope’),21,22 first results obtained in 1950. |
| 1953 | May: first trial by Hellmuth Hertz and Inge Edler on themselves of ultrasound using machine from Kockum shipyard; first A-mode scan (reflected ultrasound) of heart. |
| 1953 | 29th October, first M-mode scan by Edler and Hertz. Published 1954.23 |
| 1955 | Ian Donald (who met John Wild in London in the early 1950 s) starts to investigate reflected ultrasound in the abdomen and then in obstetric practice, like Edler and Hertz starting with a borrowed flaw detector; with engineer Tom Brown, develops ‘Diasonograph’ which produced compound obstetric scans.24 |
| 1956 | Shigeo Satomura, ultrasonic Doppler method to measure cardiac motion (with continuous wave). Initial report in Japanese,25 first publication in English in 1957.26 |
| 1960 | Tomasz Cieszyński, first intravascular scanning and intracardiac echocardiography reported, using a single-element transducer on a catheter (developed from 1956).27 |
| 1961 | Edler’s thesis published as supplement to Acta Medica Scandinavica.28 |
| 1962 | Ryozo Omoto obtained 2D intravascular images with a slowly rotating, single-element transducer mounted at a catheter tip.29,30 First publication in English in 1967.31,32 |
| 1963 | First dedicated cardiac ultrasound scanner built by John (Jack) Reid, working with cardiologist Claude Joyner.33 |
| 1963 | Olofsson develops an optical mirror system for 2D scanning of the heart,34 working with Hertz.35 Further development reported by Arne Åsberg (1967).36 |
| 1964 | ‘Ultrasono-cardio-tomography’ reported from Sendai, Japan, for 2D imaging using mechanical sector scanning.37–39 |
| 1967 | Francis McLeod, directional Doppler system.40 |
| 1967 | Jan Somer constructed first electronic phased-array scanner (‘Electroscan’).41,42 |
| 1968 | Raymond Gramiak and Pravin Shah, first report of (M-mode) contrast echocardiography.43 |
| 1968 | Daniel Kalmanson, directional flow measurement by continuous wave Doppler.44 |
| 1969 | Range-gated (pulsed) Doppler ultrasound developed by three groups: in 1969 Peter Wells45 (Bristol) and Paul Peronneau46 (Paris); and then Donald Baker47 (1970). |
| 1969 | Transthoracic (continuous wave) recording of aortic flow by Henry Light.48 |
| 1971 | Nicolaas (Klaas) Bom and Charles Lancée, first real-time 2D (linear array) cardiac scans (‘Multiscan’).49,50 |
| 1972 | Bom and colleagues, first catheter-based cylindrical phased-array ultrasonic intravascular/intracardiac transducer.51 |
| 1972 | First textbook on echocardiography (Harvey Feigenbaum).52 |
| 1973 | First clinical reports on 2D echo (using the Multiscan) by Frank Kloster53 and Jos Roelandt,54 with Bom and colleagues. |
| 1973 | James Griffith and Walter Henry, mechanical sector scanner for 2D imaging.55,56 |
| 1974 | Frederick Thurstone and Olaf von Ramm, phased-array scanner,57,58 clinical studies reported by Joe Kisslo.59 |
| 1974 | Frank Barber with John Reid, ultrasonic duplex echo-Doppler scanner.60 |
| 1974 | Prototype for 3D cardiac imaging by combining 2D images acquired in different planes (Dekker et al.).61 |
| 1974 | Louis Teichholz publishes method for calculating ejection fraction from left ventricular echocardiographic dimensions.62 |
| 1974 | Bjørn Angelsen constructed a pulsed Doppler system for recording aortic blood flow.63 |
| 1976 | Lee Frazin, single-element transoesophageal echocardiography.64 |
| 1976 | Jarle Holen, first publication using Doppler ultrasound to estimate pressure gradients in heart valve disease (using a modified Gorlin formula).65 |
| 1976 | Cees Ligtvoet with N Bom and colleagues in Rotterdam, first portable (‘hand-held’) echocardiography system (‘Minivisor’),66 clinical study published in 1978.67 |
| 1977 | Kohzoh Hisanaga, high-speed rotating cross-sectional transoesophageal scanner.68,69 |
| 1977 | Alf Brubakk with Bjørn Angelsen and Liv Hatle proposed a modified Bernoulli equation for Doppler echocardiography to assess the severity of heart valve disease.70 |
| 1978 | Marco Brandestini, multigated Doppler instrument, combining imaging of flow encoded in colour, superimposed initially on M-mode scans and later on 2D images.71–73 |
| 1978 | Griffith and Henry, combined instrument for imaging and Doppler.74 |
| 1978 | Hatle with Angelsen, quantification of mitral stenosis75 (1978) and aortic stenosis76 (1980) by the modified Bernoulli method. |
| 1979 | First report of exercise stress echocardiography using 2-dimensional imaging by Wann et al.,77 further developed by Morganroth,78 and Maurer,79 in 1981. |
| 1981 | Jacques Souquet, Peter Hanrath, transoesophageal phased-array echocardiography.80,81 |
| 1982 | First textbook on Doppler Echocardiography (Bjørn Angelsen and Liv Hatle).82 |
| 1982 | Chihiro Kasai,83 with Koroku Namekawa et al.: first commercial real-time colour flow imaging system, using autocorrelation, from Aloka; initial clinical publication by Ryozo Omoto.84 |
| 1982 | Pulsed Doppler recording of mitral flow proposed by Akira Kitabatake for the assessment of left ventricular diastolic function.85 |
| 1983 | First commercial system with colour flow mapping (Aloka). |
| 1989 | Karl Isaaz, proof of concept for regional myocardial velocity measurement.86 |
| 1991 | Olaf von Ramm, first real-time 3D imaging system (‘Volumetrics’).87 |
| 1992 | Multiplane transoesophageal echocardiography (Hewlett Packard).88 |
| 1992 | Norman McDicken and George Sutherland, development of colour and pulsed tissue Doppler (with Acuson).89 |
| 1998 | Software for imaging of regional myocardial function based on post-processing of colour tissue Doppler, by Lars-Åke Brodin and Bjørn Olstad.90 |
| 1998 | Myocardial strain rate, developed by Andreas Heimdal et al.91 |
| 2004 | Peter Lysyansky et al., first commercial system for speckle tracking of grey-scale images, leading to measurement of global longitudinal strain.92,93 |
| 2008 | Real-time ‘live’ 3D transoesophageal imaging (Lissa Sugeng et al.).94 |
| Year | Scientific contribution |
|---|---|
| 1727 | James Bradley reported the aberration of light from stars, and measured its speed.1 |
| 1738 | Daniel Bernoulli related the speed of a fluid to a local decrease in pressure or potential energy.2 |
| 1757 | Leonhard Euler (who had studied with Bernoulli’s father) published general principles of fluid dynamics,3 followed in 1775 by his publication on flow in blood that is still applicable to non-invasive haemodynamic assessments.4 |
| 1842 | Christian Doppler gave paper ‘On the coloured light of the double stars and certain other heavenly bodies’5 to the Royal Bohemian Society of Sciences, Prague, 25th May (which was a theoretical development of the earlier paper by James Bradley). |
| 1845 | Christophorus Hendrik Diederik Buijs Ballot, observed the frequency shift of sound waves.6 |
| 1880 | Jacques and Pierre Curie discovered the piezoelectric effect.7 |
| 1916 | Paul Langevin (who had been a doctoral student of Pierre Curie) developed SONAR during the First World War; he filed patents with Constantin Chilowsky in 1916 in France8 and 1917 in the USA9 (stating that ‘The relative motion of the obstacle and the observation post may be determined by applying Doppler’s method..’). |
| 1929 | Sokolov in Russia proposed using ultrasound to test castings.10 He filed a US patent application for his ultrasonic flaw detector (as Sergey Sokoloff) in 1937.11 |
| 1940 | Floyd Firestone constructed an ultrasonic reflectoscope for industrial use.12 He applied for a patent during the Second World War, and published his method afterwards in 1946.13 |
| 1942 | Karl Theo Dussik developed what he called ‘hyperphonography’, using transmitted US to examine the brain,14,15 he considered but did not pursue ultrasound reflection. |
| 1949 | Wolf-Dieter Keidel scanned the heart with transmitted ultrasound, to estimate its volume (after trying but rejecting the pulse-reflection method).16,17 |
| 1952 | John Wild and John Reid applied echo-ranging to determine the structure of biological soft tissues (including breast).18–20 Figures include ‘A-mode’ demonstration. (John Wild started his research after locating to the USA in 1946). |
| 1952 | Douglass Howry & Roderic Bliss produced compound scans of human anatomy, equivalent cumulatively to 2D cross-sections (‘Somascope’),21,22 first results obtained in 1950. |
| 1953 | May: first trial by Hellmuth Hertz and Inge Edler on themselves of ultrasound using machine from Kockum shipyard; first A-mode scan (reflected ultrasound) of heart. |
| 1953 | 29th October, first M-mode scan by Edler and Hertz. Published 1954.23 |
| 1955 | Ian Donald (who met John Wild in London in the early 1950 s) starts to investigate reflected ultrasound in the abdomen and then in obstetric practice, like Edler and Hertz starting with a borrowed flaw detector; with engineer Tom Brown, develops ‘Diasonograph’ which produced compound obstetric scans.24 |
| 1956 | Shigeo Satomura, ultrasonic Doppler method to measure cardiac motion (with continuous wave). Initial report in Japanese,25 first publication in English in 1957.26 |
| 1960 | Tomasz Cieszyński, first intravascular scanning and intracardiac echocardiography reported, using a single-element transducer on a catheter (developed from 1956).27 |
| 1961 | Edler’s thesis published as supplement to Acta Medica Scandinavica.28 |
| 1962 | Ryozo Omoto obtained 2D intravascular images with a slowly rotating, single-element transducer mounted at a catheter tip.29,30 First publication in English in 1967.31,32 |
| 1963 | First dedicated cardiac ultrasound scanner built by John (Jack) Reid, working with cardiologist Claude Joyner.33 |
| 1963 | Olofsson develops an optical mirror system for 2D scanning of the heart,34 working with Hertz.35 Further development reported by Arne Åsberg (1967).36 |
| 1964 | ‘Ultrasono-cardio-tomography’ reported from Sendai, Japan, for 2D imaging using mechanical sector scanning.37–39 |
| 1967 | Francis McLeod, directional Doppler system.40 |
| 1967 | Jan Somer constructed first electronic phased-array scanner (‘Electroscan’).41,42 |
| 1968 | Raymond Gramiak and Pravin Shah, first report of (M-mode) contrast echocardiography.43 |
| 1968 | Daniel Kalmanson, directional flow measurement by continuous wave Doppler.44 |
| 1969 | Range-gated (pulsed) Doppler ultrasound developed by three groups: in 1969 Peter Wells45 (Bristol) and Paul Peronneau46 (Paris); and then Donald Baker47 (1970). |
| 1969 | Transthoracic (continuous wave) recording of aortic flow by Henry Light.48 |
| 1971 | Nicolaas (Klaas) Bom and Charles Lancée, first real-time 2D (linear array) cardiac scans (‘Multiscan’).49,50 |
| 1972 | Bom and colleagues, first catheter-based cylindrical phased-array ultrasonic intravascular/intracardiac transducer.51 |
| 1972 | First textbook on echocardiography (Harvey Feigenbaum).52 |
| 1973 | First clinical reports on 2D echo (using the Multiscan) by Frank Kloster53 and Jos Roelandt,54 with Bom and colleagues. |
| 1973 | James Griffith and Walter Henry, mechanical sector scanner for 2D imaging.55,56 |
| 1974 | Frederick Thurstone and Olaf von Ramm, phased-array scanner,57,58 clinical studies reported by Joe Kisslo.59 |
| 1974 | Frank Barber with John Reid, ultrasonic duplex echo-Doppler scanner.60 |
| 1974 | Prototype for 3D cardiac imaging by combining 2D images acquired in different planes (Dekker et al.).61 |
| 1974 | Louis Teichholz publishes method for calculating ejection fraction from left ventricular echocardiographic dimensions.62 |
| 1974 | Bjørn Angelsen constructed a pulsed Doppler system for recording aortic blood flow.63 |
| 1976 | Lee Frazin, single-element transoesophageal echocardiography.64 |
| 1976 | Jarle Holen, first publication using Doppler ultrasound to estimate pressure gradients in heart valve disease (using a modified Gorlin formula).65 |
| 1976 | Cees Ligtvoet with N Bom and colleagues in Rotterdam, first portable (‘hand-held’) echocardiography system (‘Minivisor’),66 clinical study published in 1978.67 |
| 1977 | Kohzoh Hisanaga, high-speed rotating cross-sectional transoesophageal scanner.68,69 |
| 1977 | Alf Brubakk with Bjørn Angelsen and Liv Hatle proposed a modified Bernoulli equation for Doppler echocardiography to assess the severity of heart valve disease.70 |
| 1978 | Marco Brandestini, multigated Doppler instrument, combining imaging of flow encoded in colour, superimposed initially on M-mode scans and later on 2D images.71–73 |
| 1978 | Griffith and Henry, combined instrument for imaging and Doppler.74 |
| 1978 | Hatle with Angelsen, quantification of mitral stenosis75 (1978) and aortic stenosis76 (1980) by the modified Bernoulli method. |
| 1979 | First report of exercise stress echocardiography using 2-dimensional imaging by Wann et al.,77 further developed by Morganroth,78 and Maurer,79 in 1981. |
| 1981 | Jacques Souquet, Peter Hanrath, transoesophageal phased-array echocardiography.80,81 |
| 1982 | First textbook on Doppler Echocardiography (Bjørn Angelsen and Liv Hatle).82 |
| 1982 | Chihiro Kasai,83 with Koroku Namekawa et al.: first commercial real-time colour flow imaging system, using autocorrelation, from Aloka; initial clinical publication by Ryozo Omoto.84 |
| 1982 | Pulsed Doppler recording of mitral flow proposed by Akira Kitabatake for the assessment of left ventricular diastolic function.85 |
| 1983 | First commercial system with colour flow mapping (Aloka). |
| 1989 | Karl Isaaz, proof of concept for regional myocardial velocity measurement.86 |
| 1991 | Olaf von Ramm, first real-time 3D imaging system (‘Volumetrics’).87 |
| 1992 | Multiplane transoesophageal echocardiography (Hewlett Packard).88 |
| 1992 | Norman McDicken and George Sutherland, development of colour and pulsed tissue Doppler (with Acuson).89 |
| 1998 | Software for imaging of regional myocardial function based on post-processing of colour tissue Doppler, by Lars-Åke Brodin and Bjørn Olstad.90 |
| 1998 | Myocardial strain rate, developed by Andreas Heimdal et al.91 |
| 2004 | Peter Lysyansky et al., first commercial system for speckle tracking of grey-scale images, leading to measurement of global longitudinal strain.92,93 |
| 2008 | Real-time ‘live’ 3D transoesophageal imaging (Lissa Sugeng et al.).94 |
Note: the entries in italics concern general or non-cardiac imaging applications.
The dates refer either to the first date of use, if available, or to the earliest publication. The entries relate mostly to engineering and technical developments, rather than to the first reports of new clinical applications or insights. This timeline does not list all early investigators.
Imaging
The first successful use of reflected ultrasound to examine the heart is attributed to Inge Edler, a physician, and Hellmuth Hertz, a physicist, working in Lund in Sweden in 1953. Their initial question came from Edler, who wondered if radar could be used to study the heart. He asked for advice from Hertz,95 who was aware of the use of ultrasound for the non-destructive detection of flaws in metals. Hertz arranged to try out a scanner belonging to the Tekniska Röntgencentralen company and used at the Kockum shipyard in nearby Malmö, on himself, and then he and Edler borrowed it over a weekend. They became convinced that the ‘ultrasonic reflectoscope’ could become a valuable tool for the diagnosis of heart disease,96,97 and so they organized the loan of a machine from Siemens. Hertz devised an attachment for recording the output from its cathode ray oscilloscope, whereafter they exposed the first roll of film of an M-mode echocardiographic recording on 29th October 1953 (Figures 2 and 3). They published their initial experience in the proceedings of the Royal Physiographic Society of Lund in 1954.23 Later both Edler (personal communication) and Hertz96 recalled that at that time they had been unaware of earlier experiments with ultrasound for medical imaging.
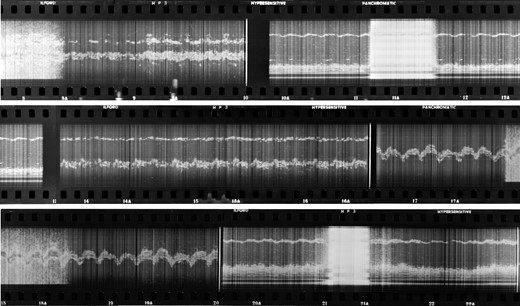
The first photographic film of M-mode echocardiography that was exposed by Edler and Hertz in October 1953, digitally scanned and then displayed as a continuous contact print. (courtesy of Professor Lars Edler)
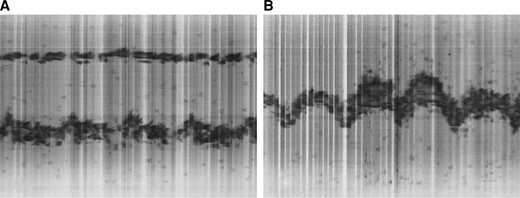
(A) frame 15; and (B) frame 19A; selected from the M-mode echocardiographic film of the heart (shown in Figure 1).
When his doctoral thesis was published as a supplement to Acta Medica Scandinavica in 1961, Edler cited earlier work by Dussik, Keidel, Wild and Reid.28 Dussik had considered using reflected rather than transmitted ultrasound to image the brain but not pursued that option.98 Keidel experimented with reflections to image the heart, but without success perhaps because of the low frequency that he was using, and so he reverted to transmitting ultrasound through the thorax.16,17,99 Elsewhere during the late 1940s, several groups in the USA were studying the properties of ultrasound in tissue,100 whereas others were studying its therapeutic potential. Experiments in Boston suggested that the varying intensities of the transmitted signals observed by Dussik and Keidel could be largely explained by absorption and attenuation. Ballantine et al.101 in the USA also referred briefly to reflected ultrasound when in 1950 they reported their investigations of the brain with transmitted ultrasound. And not long afterwards, Wild with Neal18,19 examined brain tissue in vitro and a breast lump in vivo, using reflected ultrasound at 15 MHz. He and Reid developed ‘echography’ to scan tissues; by sweeping a single ultrasonic beam mechanically across the surface of a sample, they built up a composite image.20 Similar techniques were developed by Howry & Bliss, and also reported in 1952.21,22 In a later historical account, Edler mentioned that Gohr in 1940 also proposed the use of reflected ultrasound.102,103
Edler experimented with imaging hearts obtained from autopsies, in water baths, so that he could correlate the A-mode echoes with anatomical structures. With colleagues in Lund he explored the use of the technique for possible clinical applications beyond his primary interest in assessing rheumatic mitral valve disease.104 Early visitors to their laboratory included in 1956 Sven Effert from Düsseldorf (and later Aachen), who pioneered echocardiography in Germany in the late 1950s.105–107 In general, however, Edler considered that medical colleagues were reluctant to apply their results.
Development accelerated after Edler showed a scientific film of their work at the congress of the European Society of Cardiology in Rome in 1960, and after he and Hertz had attended a symposium organized by the University of Illinois at Urbana in the USA in 1962. The method was taken up and clinical research pursued in the USA by Harvey Feigenbaum (from 1963)108 and others. The first paper published in the USA concerning cardiac ultrasound imaging had been by Wild and Reid in 1957, when they reported imaging of excised hearts,109 and Joyner and Reid published an early study on mitral valve disease in 1963.33 Edler and Hertz had called their technique ‘Ultrasound cardiography’ (or UCG, to distinguish it from the ECG) but the name ‘Echocardiography’ was proposed by Segal in 1966 and adopted by the American Institute of Ultrasound in Medicine.110,111
Feigenbaum wrote the first textbook on ‘Echocardiography’, which was published in 1972.52 He and Richard Popp compared echocardiographic measurements with left ventricular volumes estimated by angiography.112 Many other studies were performed in the early 1970s to validate M-mode measurements, including one by Popp that demonstrated the importance of using standard transducer positions.113
Two-dimensional echocardiography
Hertz had proposed cross-sectional or two-dimensional (2D) echocardiography before suitable technology was available, using a rotating mirror system (Figures 4A and 4B).34,114,115 Using this, in 1967 Åsberg reported that it produced sequences of 2D cardiac images which allowed cardiac motion to be followed.36 In addition in the mid-1960s, investigators in Japan developed a prototype mechanical sector scanner that could produce a static 2D silhoutte of the heart at any time during the heart cycle.37–39,116 That system was used by Teichholz et al. in 1974 to compare echocardiographic 2D images with biplane left ventriculography, to estimate volumes and validate their method of estimating ejection fraction from end-diastolic and end-systolic dimensions,62 while also recognizing its limitations.117
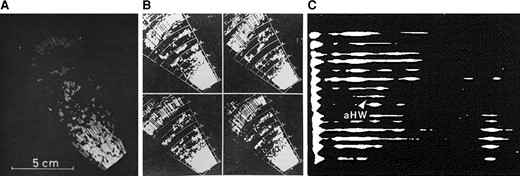
Early 2-dimensional images of the heart and mitral valve, from (A) Hertz 1964114 and (B) Hertz 1967,115 both obtained with a mirror system and recorded on 16 mm film at 7 frames per second; and (C) from Roelandt (1980; page 33)119 recorded about 1971 and described as ‘Stop-frame from the first two-dimensional ultrasonic image obtained from a patient with severe pericardial effusion; aHW = anterior heart wall.’ In this display, the transducer is along the left side of the image, and the echo-free space to the left of the arrow was interpreted as pericardial fluid in front of the heart.
The first electronic phased-array scanner was constructed by Jan Somer in 1968,41,42 and other new transducers were developed in several centres during the early 1970s.118 A linear array was made at the Thoraxcentre in Rotterdam in 1971 by Nicolaas (Klaas) Bom and Charles Lancée49,50 and used in initial clinical studies by Jos Roelandt and Frank Kloster53,54 (Figure 4C). A mechanical sector scanner was produced by Jim Griffith and Walter Henry,55,56 and a prototype phased-array scanner was built by Thurstone and Von Ramm and evaluated clinically by Joe Kisslo.57–59 Another mechanical sector scanner was developed around the same time, initially from a modified electric toothbrush, by Eggleton with Feigenbaum.120,108
These scanners were employed in the early 1970s to identify regional wall motion abnormalities during spontaneous and induced myocardial ischaemia and after myocardial infarction.121 Inducible ischaemia was diagnosed using M-mode echocardiography by several investigators during the 1970s and then exercise stress echocardiography using cross-sectional imaging was reported first in 1979.77 Others developed the technique using wider sector angles, in 1981.78,79 Pharmacological stress echocardiography using dipyridamole was proposed by Eugenio Picano and Alessandro Distante in 1985122 and stress echocardiography using dobutamine by Luc Piérard and colleagues in 1986.123
Three-dimensional echocardiography
The goal of three-dimensional (3D) imaging of the heart had been considered for a long time before progress in technology and computing could make it a realistic prospect. For example, in 1974 Dekker et al. registered the position of a probe attached to a mechanical arm, to reconstruct a 3D image after acquiring multiple 2D cross-sections.61 Others located the probe position and orientation with spark gap technology, or else they rotated the imaging plane mechanically from a stable probe position. All these original systems required external or internal reference systems to determine where the transducer was positioned in 3D space relative to the heart. Acquisition needed to be gated to the ECG, and it could take several minutes to complete an image data set encompassing the entire heart.124
The first system for true 3D echocardiographic imaging was developed by Von Ramm et al. from Duke University, North Carolina, in the early 1990s, using a sparse array.87 Their machine was very large, and despite parallel processing its frame rate was about 8/s. The first commercially available real-time 3D system using phased-array technology was released by Volumetrics in 1996. Volume rates remained slow and to create an image of the entire heart required stitching together several ECG-synchronized sub-volumes, acquired with the transducer held still while the patient held her or his breath.
Rapid advances in micro-electronics and the development of broadband (1–5 MHz) monocrystal matrix array transducers led to the development of small transducers for 3D imaging with superior sensitivity and good spatial and temporal resolution, reported clinically by Sugeng with Roberto Lang in 2003.125 Dynamic real-time transthoracic 3D imaging at high-frame rates became possible from the early 2000s, using a matrix array with 3000 elements. Colour flow images are superimposed onto the 3D tissue display in real time. More recently, post-processing techniques developed by the cartoon film industry have been applied to produce real-time ‘photo-realistic’ images. These can be illuminated by a (hypothetical) moveable light source to highlight various anatomical features, and structures can be displayed as semi-transparent.126
Transoesophageal echocardiography
In 1972 Olson and Shelton127 monitored changes in the diameter of the aortic arch in dogs using an ultrasound crystal attached to an oesophageal probe, and in 1974 Duck et al.128 reported their initial clinical experience of using a new transoesophageal ultrasonic probe to record aortic blood flow. The possibility of M-mode imaging from the oesophagus was demonstrated by Frazin et al. in 1976, using a single crystal that the patient had to swallow.64 A few years later, in New York, Masayuki Matsumoto et al. monitored left ventricular function during cardiac surgery by transoesophageal M-mode echocardiography, using a home-made system.129,130 Matsumoto then received a scholarship to spend 1 year at the Cardiology Department of the University Hospital Hamburg Eppendorf, where Peter Hanrath was working.
Although the quality of the images was good, the disadvantage of the M-mode approach was that the transducer position could not be controlled by the physician. To solve this problem, Hanrath contacted Olympus (at that time the world's leading manufacturer of flexible endoscopes) in Hamburg, and they succeeded to install a commercially available single-element transducer into the shaft of a flexible endoscope from which the fibreoptics had been removed. Their results were published in 1981131 and 1982.132
Working independently in Japan, in 1977 Hisanaga et al. had developed a rotating mechanical scanner for cross-sectional imaging of the heart from a transoesophageal approach, and also a transoesophageal-pulsed Doppler probe.68,69,133 After the initial M-mode studies in Hamburg, Hanrath searched for an ultrasound company that was able to miniaturize a phased-array transducer to such an extent that it could be built into an endoscope. In 1981, he met the engineer Jacques Souquet at Advanced Technology Laboratories (ATL) in Seattle, and about 6 months later, they delivered such a tranducer consisting of 36 crystals, which was then incorporated into an endoscope by Olympus. The resulting first clinical studies of monoplane transoesophageal imaging (Figure 5) were published in 1982.80,81 This was followed soon afterwards by their development of a biplane transducer.134 Further developments were also taking place in Japan.135
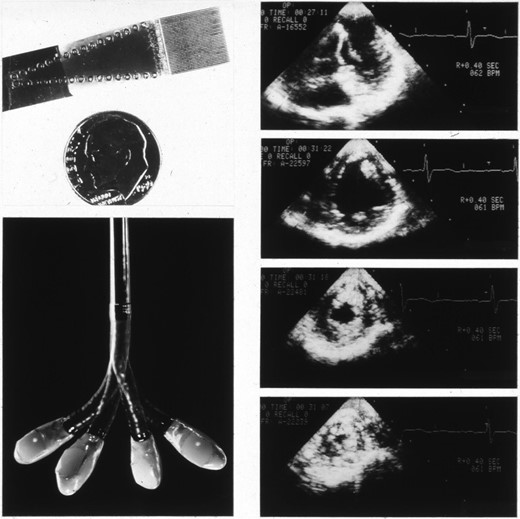
Early monoplane transoesophageal probe and images (courtesy of Professor Peter Hanrath).
Souquet and Hanrath had the idea of a rotatable phased-array transducer in an endoscope, which at that time represented a constructional challenge. They submitted a joint grant application to the German Ministry of Research and Technology in 1982, but it was rejected with the argument that German tax money could not be spent to support American industry. In 1989, Hanrath met engineers from Hewlett Packard in Boston, who felt able and willing to develop a rotatable multiplane probe—but first, legal action was needed to revoke a patent that had in the meantime been claimed by Souquet. Thereafter a prototype multiplanar (or ‘Omniplane’) probe was delivered to Hanrath (by then in Aachen) from Hewlett Packard in 1991, and their initial clinical experience was published soon afterwards.88 ln the same year (1992), the Rotterdam group published their first clinical results with another multiplane transoesophageal probe, that they had also developed with Hewlett Packard, called the ‘Varioplane’.136
A paediatric single-plane 5.0 MHz transoesophageal probe was developed by the Oldelft company in 1989, working with engineers at the Thoraxcentre in Rotterdam.137 A series of correlative clinical reports confirmed the additional clinical value of transoesophageal imaging in congenital heart disease.138,139 This was followed by the development of biplane and then steered matrix multiplane paediatric transoesophageal probes. In adults, the first clinical report of real-time 3D transoesophageal imaging using a matrix transducer was published in 2008.94 Now, high-quality 3D transoesophageal images can be fused in real-time with fluoroscopic images, to guide cardiac structural interventions by visualising catheters, contrast, tissue structures and blood flow, all spatially synchronized and superimposed.
Doppler ultrasound
There is a long history of the development of ultrasonic methods for recording and displaying blood flow and measuring its velocity in order to derive estimates of intracardiac pressure gradients. Although we apply the name of Christian Doppler, his original presentation in Prague in 18425 was a theoretical development of an earlier study on the motion of distant stars by James Bradley,1 without any new or original experimental observations.140 A change in the frequency of sound waves as they are transmitted from a moving target or towards a travelling observer, was first demonstrated a few years later in the Netherlands by Christophorus Buijs Ballot who arranged for a train to travel past stationary musicians playing a constant note on a horn.6 He had been sceptical and was trying to disprove Doppler’s hypothesis but in fact confirmed it.140,141
Cardiovascular imaging applications now estimate velocities using autocorrelation to assess phase shift,142 rather than by calculating the Doppler shift in frequency or wavelength, but the eponymous attribution persists. Doppler echocardiography was developed during the 1950s in Japan by Shigeo Satomura, whose first investigations from 1952 were to measure heart motion rather than blood flow.25,27,143 In 1956 Yoshida with Satomura reported that Doppler ultrasound signals could be obtained from the human heart due to the motion of heart valves and blood flow.144,145 Other Japanese investigators correlated the observed phase shift with the velocity of the target, and related the amplitude of the signal to the number of red cells as reflectors.146,147
In 1966 and independently, both Kato in Japan and Robert Rushmer in the USA reported that they had developed directional blood flow meters.148,149 A prototype apparatus for the continuous assessment of flow was also reported by Francis McLeod in 1967,40 and another by Daniel Kalmanson in Paris in 1968 with the engineer Gérard Toutain.44,150 These machines recorded directional Doppler signals, meaning that it was possible to distinguish blood flow towards or away from the transducer, for example in the jugular vein of patients with right heart disease.151 About the same time, Light was using Doppler from a suprasternal approach to record aortic blood flow.48 More significantly, range-gated or pulsed Doppler was being developed independently by three groups—Peter Wells in Bristol45 and Paul Peronneau in Paris,46 both reported in 1969, and Donald Baker in Seattle, published in 1970.47 Thereafter the key advance was the development of a duplex scanner by Frank Barber in 1974, so that images and flow could be recorded using a single ultrasound system.60 Griffith and Henry published details of another combined system in 1978.74 Thus far, blood flow in the heart and vessels could be assessed only semi-quantitatively.152
The first person to demonstrate (in 1976) that Doppler measurements of intracardiac flow velocities could be used to estimate pressure gradients was Jarle Holen, who had worked as an aerodynamics engineer at the Boeing factory in Seattle before studying medicine. He went from Rochester in New York state, where he had worked in the radiology department with Gramiak, to Oslo to undertake his doctoral research. At first, the university department did not have an echocardiographic machine, and so a foetal monitor was modified to obtain Doppler signals. He then measured the velocity of flow across the mitral valve in patients with stenosis and calculated the gradients by an application of the Gorlin formula; the results correlated well with invasive measurements.65 Some years later, in an in vitro experiment, he confirmed the accuracy of the new methods against pressures that were measured directly.153
Independently, and from about 1974, Bjørn Angelsen at the Norwegian Technical University in Trondheim developed a combined pulsed and continuous wave Doppler system63,154 and proposed that gradients could be estimated using a simplification of the Bernoulli equation.70 Liv Hatle was provided with a system built by Kjell Kristoffersen from Angelsen’s group, and their first clinical study was presented by Brubakk at the European Congress of Cardiology in Amsterdam in 1976; it was met with some disbelief but Holen’s paper came out shortly afterwards, confirming the results. Seminal publications followed from 1978 on the quantification of mitral stenosis,75 aortic stenosis,76 tricuspid regurgitation,155 and right ventricular systolic pressure.156 Investigators in Japan proposed that mitral and tricuspid flow velocities could be used to estimate left and right ventricular diastolic filling and function.85,157
Colour flow mapping became possible after the development of a multigate pulsed Doppler system, first reported in the late 1970s by the engineer Marco Brandestini from Don Baker’s group at the University of Washington in Seattle.71,72 His initial prototype superimposed colour flow on M-mode echocardiography, but it was soon followed by colour flow on a 2D display.73 The first commercially available system was developed at the Aloka company in Japan, by the engineer Chihiro Kasai et al., from 1982 and in collaboration with Ryozo Omoto who reported their initial clinical experience in 1984.83,84,158 In the same year, Rolf Jenni used a Diasonics multigate Doppler system to reveal varying flow patterns across the human aorta.159
Myocardial velocity imaging
The proof of concept for recording a Doppler signal from the myocardium came from Isaaz in 1989,86 after earlier attempts with related but different techniques by Yoshida145 and Kostis.160 The key advance was the development of a method by McDicken and Sutherland which adapted the colour Doppler algorithms for flow in a standard echocardiographic machine preferentially to display the high-amplitude, low-velocity signals from the myocardium.89,161 This was soon integrated into commercially available imaging systems by the Acuson company (as ‘Doppler myocardial imaging’) during the 1990s. A method was proposed for the post-processing of colour Doppler information to derive maps of other features of regional myocardial function,90 and then methods were demonstrated for measuring local deformation of the myocardium as strain rate or strain.91 Doppler myocardial Imaging was introduced into paediatric cardiology from 2002.162,163
Tracking the speckle pattern of ultrasound reflections, to obtain angle-independent images of blood flow and tissue motion, was suggested in 1991 but not feasible for implementation at that time because of insufficient computing capacity.164 The first practical solution that became commercially available was developed by the General Electric company in Israel by the engineer Peter Lysyansky with clinical colleagues, in 2004.92,93 Although now widely applied, the technique has insufficient temporal resolution to fully resolve regional myocardial strain rates.
Echocardiography in congenital heart disease
Following the introduction of low frequency (2.5 MHz) M-mode echocardiography into adult cardiology in the late 1960s, it was used at higher imaging frequencies (5.0 and 7.5 MHz) to study cardiac structure and function in children with congenital or acquired heart lesions. Whereas the anatomy of the cardiac chambers and vascular connections in most adults is predictable, the geometry of complex congenital malformations posed a great challenge for the M-mode technique. Despite this caveat, early diagnostic studies were reported in 1967165 and 1971.166 At that time the morphology of complex congenital cardiac lesions was poorly understood, but certain patterns on M-mode traces were described which could suggest underlying structural malformations such as transposition of the great arteries.167 Nonetheless, the limitations of the M-mode technique for describing spatially complex lesions rapidly became evident.
Pioneering work on cardiac morphology by the Van Praaghs in the 1960s168 and the Anderson group in the 1970s169 was crucial for understanding and defining complex congenital cardiac malformations. By the early 1990s a series of studies had correlated echocardiographic findings with morphology, aided by the introduction of 5.0 and 7.5 MHz mechanical and phased-array 2-D imaging systems and by the development and integration of Doppler ultrasound modalities.170,171 Together, these led to the acceptance of cardiac ultrasound as a comprehensive and accurate modality to diagnose complex congenital heart disease.172
Paediatric 2D sector scanning had been developed separately and in parallel with pulsed and continuous wave Doppler modalities, during the late 1970s. At first, the most successful systems were the mechanical rotational sector scanners developed by ATL, that imaged at 3.5 to 7.0 MHz. In parallel, Bjørn Angelsen and Kjell Kristoffersen63,154 developed their non-imaging pulsed and continuous wave Doppler system (which they called a pulsed-echo Doppler flowmeter, or PEDOF).63,154 It was tested clinically by Hatle and colleagues in Trondheim in 1976, and applied for the first non-invasive haemodynamic study of ventricular septal defects.173 In 1982, the large Irex 111B duplex scanner was introduced, which for the first time combined 2D sector scanning with pulsed and continuous wave Doppler modalities.
Clinically effective colour flow mapping (CFM) was integrated into paediatric scanners by the mid 1980s, but again by two differing approaches. Vingmed (1986) and ATL based their CFM on rotational mechanical sector scanners, while Aloka (1987) introduced high-frequency phased-array scanners that imaged at 5.0 and 7.5 MHz. By the early 1990s, improvements in transducer ceramic materials allowed more crystals to be mounted, to produce an electronically steered matrix 2D array. Allied with new digital monitors and software-driven digital ultrasound machines, data could be acquired at high transducer frequency and displayed with high temporal and spatial resolution. These developments, combined with commercial considerations, led to the demise of mechanical sector scanners. Improvements in paediatric matrix probes, probe bus data transfer and machine processing speed, and digital displays, enabled real-time 3D transthoracic and transoesophageal echocardiography to be introduced to paediatric practice from the mid 2000s.174,175
Foetal echocardiography
Ultrasound examination of the foetal heart was first described in 1966, using M-mode echocardiography,176,177 but it did not come of age until full integrated paediatric 2D ultrasound scanners became available from the late 1970s. Starting in 1980, Lindsey Allan produced a series of innovative reports on the intrauterine diagnosis of congenital heart disease, using both mechanical and phased-array sector scanners.178 Once initial safety fears for the foetus had been addressed, this led to the widespread acceptance of trans-abdominal and trans-vaginal foetal echocardiography. New ultrasound modalities have been incorporated, including the assessment of intracardiac flows, myocardial deformation, and 3D imaging. Foetal echocardiography has become established as an essential discipline shared with obstetricians.
Intravascular ultrasound
In 1956, Tomasz Cieszyński built an ultrasonic catheter with the goal of applying it for intracardiac investigations, but his initial article reported experimental studies only (in vitro and in animals).27 Dean Franklin’s group at the University of Washington, Seattle, described an invasive ultrasound flowmeter in 1959, but it was clamped around the aorta rather than being intravascular and it was also assessed in animal experiments.179 More studies were conducted by Ryozo Omoto et al.29–31,180 in Japan, while independently in Rotterdam in the early 1970s Bom et al.51 developed their first intravascular phased-array transducer, with 32 elements (Figure 6). Kalmanson recorded intracardiac signals from the right and left heart in 1979 and 1980, using directional Doppler.152
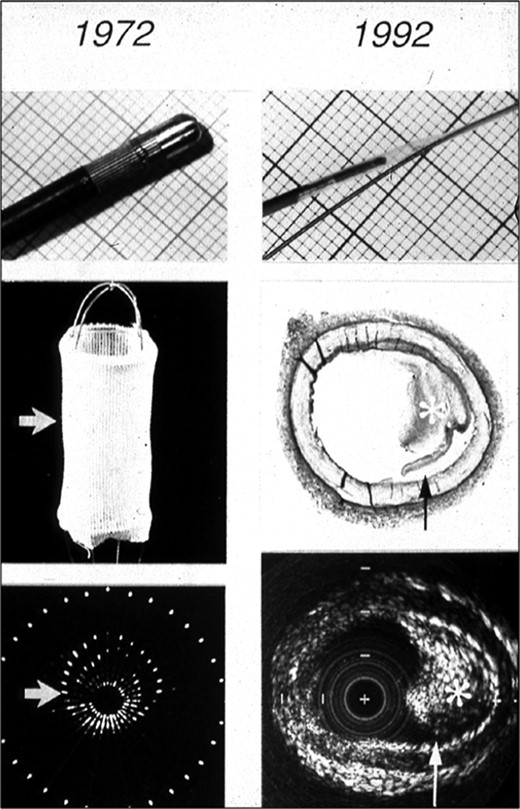
Left: 32-element phased-array 5.6 MHz intravascular ultrasound imaging (IVUS) of a basket (1972). Right: Single element rotating 30 MHz IVUS image of an artery containing atherosclerotic plaque (asterisk, and arrowed) (1992). From Bom N, Lancée CT, Rijsterborgh H, ten Hoff H, Roelandt JRTC. From idea to clinical application. in Intravascular Ultrasound, Roelandt, Gussenhoven, Bom Eds. Kluwer Academic Publishers, 1993.
After initial enthusiasm, interest in intravascular ultrasound (IVUS) was stalled until the mid 1980s when clinical impetus was provided by the development of percutaneous coronary interventions and by recognition that the X-ray shadow image of the lumen provided too limited information to develop balloon angioplasty, atherectomy, spark erosion, and other techniques safely. For that reason, IVUS was developed further.181 Bom et al. made a combined IVUS/spark erosion catheter and demonstrated its feasibility in vitro in 1988.182 Later, it was developed as a standalone IVUS system. In 1989 Paul Yock introduced a clinical rotating IVUS system, initially for imaging peripheral arteries and then for intracoronary imaging.183 Its clinical application was confirmed for evaluating atherectomy and laser ablation.184 Tobis et al. evaluated balloon angioplasty in vitro, using IVUS.185 In addition in 1989, Hodgson introduced a clinical intracoronary phased-array imaging system, based on the 1972 patent from Bom and Lancée.186
Backscatter analysis187 and lessons learned from the analysis of images obtained in vitro188 have played a major role in aiding the interpretation of IVUS images. Li et al.189 developed semi-automatic lumen detection that was applied to assess the long-term effects of several stenting strategies and to compare the efficacy of statins. Several strategies for tissue identification have emerged, but none has yet been implemented into routine clinical practice. More recently, several ‘sound and light combination’ catheters have been developed, including an IVUS NIRS catheter (near-infrared spectroscopy) by InfraredX in collaboration with van der Steen and Serruys.190
Conclusions
Although we have tried to locate and cite as many ‘first’ publications as possible, any retrospective exercise such as this is fraught with risks of inappropriate attributions or errors of omission. To minimize these, we have consulted the original publications and reviewed their reference lists, and when possible we have confirmed details with senior colleagues. We also reviewed historical accounts that have been published by principal investigators, which have been cited so that they can be consulted for more comprehensive details. Parallel developments in applications of ultrasound in other clinical fields have been reviewed recently by the European Federation of Societies of Ultrasound in Medicine and Biology,191 and other first-hand accounts of specific aspects of the history of echocardiography are available.192–194
This endeavour has reinforced the view that it is often very difficult to establish scientific precedence. Clinical advances in echocardiographic imaging have been absolutely dependent on advances in technology, and when the intellectual climate was ripe and practical tools were available then many engineers and clinicians tackled similar challenges. There have been frequent occasions in the early history of ultrasound imaging when investigators were trying to solve the same problems but communication was less easy than now and publications were less accessible, and so they worked independently. As we have summarized, many individuals who are most prominently associated with particular developments have not been the first in their field. If that was part of the reasoning behind decisions not to award the Nobel prize for medicine to Edler and Hertz, then it may become apparent once the committee’s deliberations are made available for review by historians after the usual 50-year embargo.
A second and obvious conclusion is that major advances have come from close collaborations between engineers and clinical scientists, so there is a need to ensure that such environments are developed and appropriately resourced. Although some researchers may be strongly motivated by competition, and careers can now be determined by metrics of academic productivity, in our opinion the most successful innovations have occurred when colleagues from different disciplines and different centres have been working together, preferably with an open and generous exchange of ideas. From an historical perspective what may be most interesting to current researchers is not what was done or by whom, but how the ideas and hypotheses were developed and where the original concepts came from—which is less often documented for posterity.
We have concentrated on describing the history of technological advances rather than clinical applications (Graphical Abstract), because that would have been an almost impossible undertaking. For practical reasons also, we have only briefly summarized the first steps in IVUS, which evolved from cardiac imaging but has now developed into an interventional subspecialty, and we have not reviewed vascular ultrasound or the development of hand-held systems. Echocardiography is still operator-dependent but that will lessen as machine learning methods are developed and implemented for acquiring, optimising, identifying and measuring images more accurately and reproducibly. Faster data transfer and processing would enhance the quality of 3D imaging and flow acquisition to such an extent that it could become standard practice, with all 2D, deformation and flow images and measurements being derived during post-processing, together with automated measurement of most parameters. While advances in software and artificial intelligence may transform clinical practice, it is too soon to include them in an historical overview. Similarly in our opinion the clinical utilities of recent technological developments such as high-frame-rate or ultrafast imaging, tissue characterisation by elastography, and the imaging of fluid dynamics, are still uncertain.
For the future, it could be particularly useful to establish some mechanism for expert clinical practitioners to reach a consensus on genuine unmet needs, since that has always been difficult and prone to individuals’ expertise, interests and biases. As Henry Light wrote in 1992, what will be used may involve ‘surrendering the ultimately desirable for the robustly measurable and eminently useful,’195 which implies a need for more epidemiological and outcomes-based evaluations. And hopefully, dialogue between clinicians and engineers may overcome the problem identified by Hertz in 1973 that ‘.. different physicians had very different opinions on the relative importance of possible additional features and no clear answer could be given to the designing engineers in industry’.96
Acknowledgements
We thank Professor Christoph Dietrich, European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB), for proposing this historical summary, and we acknowledge our gratitude to the late Professor Jos RTC Roelandt for stimulating our interest in the history of cardiovascular ultrasound. We thank Professors Liv Hatle, Peter Hanrath, and Alessandro Distante for their helpful suggestions concerning historical details; Professors Nicolaas Bom, Alan Pearlman, and Randolph Martin for reviewing the manuscript; Dr Sayuri Yoshioka, The Cardiovascular Institute Hospital, Tokyo, and Professor Yoshifumi Saijo, Graduate School of Biomedical Engineering, Tohoku University, Sendai, for their support in reviewing Japanese publications; and Professor Piotr Szymański, Clinical Cardiology Centre, Central Clinical Hospital MSWiA, Warsaw, for checking the Polish citation.
Funding
No external funding.
References
Author notes
Conflict of interest: None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}