





Abstract
To investigate differences in the prevalence of left ventricular (LV) and left atrial (LA) remodelling in hypertensive patients using various thresholds defined by international guidelines and data from the Echocardiographic Measurements in Normal Chinese Adults (EMINCA) study and different indexation methods.
LV mass (LVM), relative ventricular wall thickness, and LA volume (LAV) were measured using 2D echocardiography in 612 healthy volunteers selected from the EMINCA study population and 306 adult Chinese patients with hypertension who were age- and gender-matched using propensity score-matched analysis. LVM and LAV values were indexed to body surface area (BSA), height2.7, height1.7, and height2 recommended by guidelines or investigators. Using a previously reported method, LV geometry was divided into normal geometry, concentric remodelling, eccentric hypertrophy, and concentric hypertrophy. The prevalence of LV hypertrophy (LVH) and LV geometric patterns in hypertensive patients were compared using different thresholds and indexation methods. Echocardiographic thresholds from guidelines and healthy volunteers exhibited notable differences, particularly for LAV indexed to height2 and for LVM indexed to height1.7, which resulted in a significantly lower prevalence of LA dilatation and LVH in healthy volunteers. The total proportion of abnormal LV geometric patterns was significantly lower with thresholds from healthy volunteers than from guidelines when LVM was indexed to BSA, height1.7, and height2,7.
Using current echocardiographic thresholds and indexing methods recommended by guidelines may lead to significant misdiagnosis of LA dilatation, and abnormal LV geometry in Chinese patients with hypertension, and thresholds based on ethnic-specific normal echocardiographic reference values and an accurate indexing algorithm are warranted.

Introduction
Recent epidemiological studies showed that hypertension is a major risk factor that contributes to mortality and morbidity in the Chinese population.1 It has been well-documented that poorly controlled hypertension may lead to left ventricular hypertrophy (LVH), an independent risk factor for cardiovascular morbidity and mortality.2,3 In addition to an increased left ventricular mass (LVM), hypertension may lead to a spectrum of left ventricular (LV) geometric patterns. In 1990, Ganau et al.4 provided the first description of LV geometric patterns in patients with hypertension. Based on echocardiographic measurements of LVM and relative wall thickness (RWT), they outlined four patterns: normal geometry, concentric remodelling, concentric hypertrophy, and eccentric hypertrophy. Subjects with concentric remodelling and concentric hypertrophy were reported to have a higher risk for adverse cardiovascular events.5,6 Subsequent studies demonstrated that these geometric patterns were associated with different LV function status and loading conditions,7 and early intervention to prevent or reverse LV remodelling could reduce cardiovascular events.8–10 As a result, the American Society of Echocardiography (ASE) and the European Association of Cardiovascular Imaging (EACVI) recommended the description of LV geometry as a standard component of the echocardiography report in 2015.11,12 In addition, as the Framingham Heart Study revealed that left atrial (LA) dilatation was related to blood pressure and LVM,13 measurement of LA volume (LAV) was recommended for evaluating LA remodelling in the ASE/EACVI guidelines.11,12
To achieve an accurate description of LV and LA geometry, it is necessary to use standard echocardiographic techniques and well-defined thresholds. Although the ASE/EACVI guidelines have done an excellent job in standardizing image acquisition, measurement and analysis, normal LVM, RWT, and LAV reference values, as well as thresholds for identifying abnormal values, are primarily derived from Caucasians.11,12 However, in the Echocardiographic Measurements in Normal Chinese Adults (EMINCA) study, a prospective, multicentre, nationwide study, most 2D echocardiographic parameters exhibited smaller values in both sexes than those recommended by the ASE/EACVI guidelines.14 This inspired the design and execution of the World Alliance Societies of Echocardiography (WASE) Normal Values study. An important finding of the WASE study was that the normal values of most 2D echocardiographic parameters differed significantly among different races and countries.15 These studies raised important questions. Are the diagnostic thresholds for LV and LA remodelling and classification criteria of LV geometric patterns in hypertensive patients recommended by the ASE/EACVI guidelines applicable to the Chinese population? If not, what are the applicable thresholds and criteria for Chinese patients with hypertension? This study was designed and conducted to address these questions. We compared LV and LA echocardiographic values from the EMINCA database to a group of Chinese patients with hypertension using different thresholds defined by international guidelines and EMINCA data and using different indexation methods.
Methods
Study population
Chinese healthy volunteers and patients with hypertension were included in this study. The healthy volunteer group included 612 healthy Chinese Han volunteers who were selected from the EMINCA study population by matching age and gender with hypertensive patient group using propensity score-matched analysis, who met the inclusion and exclusion criteria defined in the EMINCA study.14 The inclusion criteria required that all volunteers be aged 18–79 years, have Han nationality, have normal blood pressure [systolic blood pressure (SBP) < 140 mmHg, diastolic blood pressure (DBP) < 90 mmHg], have normal results on physical examination and electrocardiography, and have no history of cardiovascular diseases. The exclusion criteria were coronary artery disease, structural heart disease, heart failure, hypertension, stroke, hyperlipidaemia (serum total cholesterol ≥ 5.72 mmol/L or triglyceride ≥ 1.70 mmol/L), diabetes mellitus (fasting blood glucose > 7.0 mmol/L), and any other endocrine diseases, acute or chronic respiratory diseases, anaemia, connective tissue disease, abnormal liver function (serum alanine aminotransferase or aspartate aminotransferase > 2.0 times the upper limit of normal), abnormal renal function (serum creatinine > 2 mg/dL), obesity [body mass index (BMI) ≥ 28.0 kg/m2], abnormal results on electrocardiography, valvular stenosis, more than mild valvular regurgitation, or wall motion abnormalities on echocardiographic recordings. Professional athletes, pregnant or lactating women, subjects addicted to alcohol, and subjects with inadequate echocardiographic images were also excluded.14 The hypertensive patients were recruited from Department of Cardiology, Shandong University Qilu Hospital from October 2016 to February 2019, who met the following inclusion and exclusion criteria. The inclusion criteria were: (i) patients with a history of hypertension; (ii) patients with elevated blood pressure measured three times on different days with SBP ≥140 mmHg and/or DBP ≥90 mmHg in the absence of antihypertensive treatment; (iii) patients with blood pressure lower than 140/90 mmHg if antihypertensive medications were being used; and (iv) patients with sinus rhythm during the echocardiographic examination. The exclusion criteria were: (i) patients with a history of myocardial infarction, significant valvular heart disease, congenital heart disease, cardiomyopathy, heart failure, atrial fibrillation, and systemic disease; (ii) patients with a poor echocardiography imaging quality. A total of 306 hypertensive patients were finally recruited. The study protocol was approved by the Ethics Committee of Shandong University Qilu Hospital (Ethics approval number: 2017087), and written informed consent was obtained from all participants.
Echocardiographic examination
Echocardiographic examination was performed using the Phillip EPIQ7C system (Philips Ultrasound, Bothell, WA, USA) connected with an S5-1 probe (1.0–5.0 MHz) or the Hitachi Aloka Prosound F75 system (Hitachi-Aloka Ultrasound, Tokyo, Japan) connected with a UST-52105 probe (1.0–5.0 MHz). LA and LV parameters were measured using standard 2D echocardiography according to the ASE/EACVI guidelines issued in 2015.12 Interventricular septal end-diastolic thickness (IVSTd), LV posterior wall end-diastolic thickness (LVPWTd), and LV end-diastolic diameter (LVEDD) were measured from the parasternal long-axis view at the level of the mitral valve leaflet tips (Figure 1). LVM was calculated with the formula: LVM = 0.8 × 1.04× [(IVSTd + LVEDD + LVPWTd)3 − LVEDD3] + 0.6 g.11,12,14 LA size was measured at ventricular end-systole, when the LA chamber is largest during the cardiac cycle. LAV and LV ejection fraction were measured in the apical four- and two-chamber views using the biplane Simpson method (Figure 1). To avoid the effect of the bulging basal portion of the interventricular septum commonly observed in elderly people, RWT was calculated using the following formula: RWT = (LVPWTd × 2)/LVEDD, which was proposed by Ganau et al.4,11,12 in their original study of classification of LV geometric patterns and later on adopted by the ASE/EACVI guidelines. Body surface area (BSA) was calculated using the Du Bois formula,16 and BMI was calculated by dividing weight in kilograms by the square of height (H) in metres. The echocardiographic values of LVM were indexed to BSA or H2.7 based on the ASE/EACVI recommendations,11,12 and those of LAV were indexed to BSA or H2 in accordance with the ASE/EACVI and the European Society of Cardiology (ESC) and European Society of Hypertension (ESH) recommendations.11,17 As the appropriate indexation of LVM remains an issue of contention, we also used another indexation method by Chirinos et al.18 who proposed to index LVM to H1.7. The thresholds of LVPWTd, LVEDD, and LAV for differentiating abnormality from normality were derived from the mean + [1.96 × standard deviation (SD)] of the normal reference values of the selected healthy volunteers in the EMINCA study population, and recommended by the ASE/EACVI or ESC/ESH guidelines.11,12,17
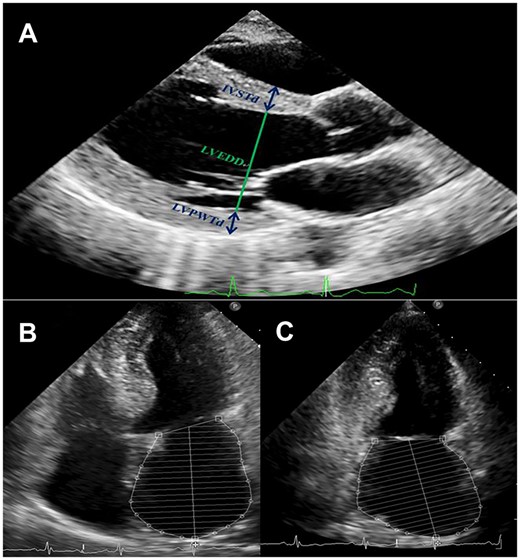
Measurement of left ventricular and left atrial echocardiographic parameters. (A) A representative parasternal long-axis view showing the method for measuring IVSTd, LVEDD, and LVPWTd at end-diastole. (B) A representative apical four-chamber view showing the method for measuring LAV at end-systole using biplane Simpson’s algorithm. (C) A representative apical two-chamber view showing the method for measuring LAV at end-systole using biplane Simpson’s algorithm. IVSTd, interventricular septum thickness at end-diastole; LAV, left atrial volume; LVEDD, left ventricular end-diastolic diameter; LVPWTd, left ventricular posterior wall thickness at end-diastole.
Classification of LV geometric patterns
Proposed initially by Ganau et al.4 and later recommended by the ASE/EACVI guidelines,11,12 LV geometric patterns in patients with hypertension are classified into four categories according to the relationship between LVM and RWT: (i) concentric hypertrophy: increased LVM and increased RWT; (ii) eccentric hypertrophy: increased LVM and normal RWT; (iii) concentric remodelling: normal LVM and increased RWT; and (iv) normal geometry: normal LVM and normal RWT.
Interobserver and intraobserver variability
To test the reproducibility of echocardiographic measurements, four key parameters, including IVSTd, LVEDD, LVPWTd, and LAV, were remeasured in 30 randomly selected subjects from the hypertensive patient group. Interobserver variability was assessed between two investigators of this study (Y.S. and Y.H.) and intraobserver variability was assessed by Y.S. Bland–Altman analysis was used to assess interobserver and intraobserver variability, and interclass correlation coefficients were calculated.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics 20.0 software (IBM Corporation, Armonk, NY, USA). The Kolmogorov–Smirnov method was used to test the normality distribution of all continuous variables. If a raw or log-transformed variable was normally distributed, it was expressed as mean ± 1.96 SD. If the raw variable or log-transformed variable was not normally distributed, it was presented as the range between the 2.5th and 97.5th percentiles. Continuous variables are expressed as mean ± SD and categorical variables as number and percentage. When the data conformed to a normal distribution, two groups were compared using the paired t-test, and multiple groups were compared using single-factor analysis of variance. Non-parametric tests were used for analysing data that were not normally distributed. Composition ratios were compared using the χ2 test. Propensity score matching analysis was performed with ‘MatchIt’ package from R software version 4.0.4 (R Foundation for Statistical Computing, Vienna, Austria) and a 2:1 ratio of the EMINCA population and hypertensive patients was adopted with the nearest neighbour method of the propensity score to match age and sex between the two groups. Bland–Altman analysis was applied to assess interobserver and intraobserver variability of echocardiographic measurement. P < 0.05 was considered statistically significant.
Results
Baseline characteristics of the study population
Baseline characteristics of the healthy volunteer group and hypertensive patient group are listed in Table 1. The healthy volunteer group included 332 men aged 54.38 ± 10.79 years and 280 women aged 60.26 ± 9.93 years and the hypertensive patient group comprised 181 men aged 55.56 ± 10.62 years and 125 women aged 58.98 ± 9.21 years. All patients in the hypertensive patient group had a history of hypertension and received one or two classes of antihypertensive medications. There was no significant difference in age, proportion of males, and height between the two groups. However, all blood pressure and echocardiographic parameters showed higher values in the hypertensive patient group than the healthy volunteer group except for heart rate and LVEDD/BSA (Table 1).
Baseline characteristics and echocardiographic measurements in healthy volunteers selected from the EMINCA study population and hypertensive patients (mean ± SD)
| Healthy volunteers (n = 612) | Hypertensive patients (n = 306) | P-value | |
|---|---|---|---|
| Age (years) | 57.07 ± 10.80 | 56.95 ± 10.19 | 0.874 |
| Sex, male | 332 (54.2%) | 181 (59.2%) | 0.159 |
| Height (cm) | 166.13 ± 8.19 | 166.22 ± 7.62 | 0.874 |
| Weight (kg) | 64.59 ± 9.35 | 73.10 ± 12.87 | <0.001 |
| BMI (kg/m2) | 23.31 ± 2.09 | 26.36 ± 3.67 | <0.001 |
| BSA (m2) | 1.75 ± 0.16 | 1.81 ± 0.18 | <0.001 |
| SBP (mmHg) | 120.65 ± 9.82 | 146.87 ± 17.43 | <0.001 |
| DBP (mmHg) | 76.43 ± 7.10 | 87.18 ± 12.82 | <0.001 |
| HR (bpm) | 71.98 ± 8.33 | 71.72 ± 11.34 | 0.725 |
| IVSTd (mm) | 8.88 ± 1.32 | 11.44 ± 1.62 | <0.001 |
| LVEDD (mm) | 45.04 ± 4.06 | 45.36 ± 4.28 | 0.270 |
| LVEDD/BSA (mm/m2) | 25.92 ± 2.63 | 25.21 ± 2.62 | <0.001 |
| LVPWTd (mm) | 8.59 ± 1.25 | 10.11 ± 1.37 | <0.001 |
| RWT | 0.38 ± 0.06 | 0.45 ± 0.07 | <0.001 |
| LVM (g) | 129.65 ± 32.23 | 174.73 ± 42.45 | <0.001 |
| LVM/BSA (g/m2) | 74.21 ± 17.02 | 96.36 ± 20.23 | <0.001 |
| LVM/height2.7 (g/m2.7) | 32.99 ± 7.95 | 44.20 ± 9.67 | <0.001 |
| LVM/height1.7 (g/m1.7) | 54.67 ± 12.83 | 73.41 ± 16.18 | <0.001 |
| LVEF (%) | 65.12 ± 6.02 | 65.75 ± 6.55 | 0.153 |
| LAV (mL) | 38.43 ± 11.49 | 50.09 ± 13.10 | <0.001 |
| LAV/BSA (mL/m2) | 22.11 ± 6.61 | 27.87 ± 7.44 | <0.001 |
| LAV/height2 (mL/m2) | 14.02 ± 4.30 | 18.25 ± 4.96 | <0.001 |
| Healthy volunteers (n = 612) | Hypertensive patients (n = 306) | P-value | |
|---|---|---|---|
| Age (years) | 57.07 ± 10.80 | 56.95 ± 10.19 | 0.874 |
| Sex, male | 332 (54.2%) | 181 (59.2%) | 0.159 |
| Height (cm) | 166.13 ± 8.19 | 166.22 ± 7.62 | 0.874 |
| Weight (kg) | 64.59 ± 9.35 | 73.10 ± 12.87 | <0.001 |
| BMI (kg/m2) | 23.31 ± 2.09 | 26.36 ± 3.67 | <0.001 |
| BSA (m2) | 1.75 ± 0.16 | 1.81 ± 0.18 | <0.001 |
| SBP (mmHg) | 120.65 ± 9.82 | 146.87 ± 17.43 | <0.001 |
| DBP (mmHg) | 76.43 ± 7.10 | 87.18 ± 12.82 | <0.001 |
| HR (bpm) | 71.98 ± 8.33 | 71.72 ± 11.34 | 0.725 |
| IVSTd (mm) | 8.88 ± 1.32 | 11.44 ± 1.62 | <0.001 |
| LVEDD (mm) | 45.04 ± 4.06 | 45.36 ± 4.28 | 0.270 |
| LVEDD/BSA (mm/m2) | 25.92 ± 2.63 | 25.21 ± 2.62 | <0.001 |
| LVPWTd (mm) | 8.59 ± 1.25 | 10.11 ± 1.37 | <0.001 |
| RWT | 0.38 ± 0.06 | 0.45 ± 0.07 | <0.001 |
| LVM (g) | 129.65 ± 32.23 | 174.73 ± 42.45 | <0.001 |
| LVM/BSA (g/m2) | 74.21 ± 17.02 | 96.36 ± 20.23 | <0.001 |
| LVM/height2.7 (g/m2.7) | 32.99 ± 7.95 | 44.20 ± 9.67 | <0.001 |
| LVM/height1.7 (g/m1.7) | 54.67 ± 12.83 | 73.41 ± 16.18 | <0.001 |
| LVEF (%) | 65.12 ± 6.02 | 65.75 ± 6.55 | 0.153 |
| LAV (mL) | 38.43 ± 11.49 | 50.09 ± 13.10 | <0.001 |
| LAV/BSA (mL/m2) | 22.11 ± 6.61 | 27.87 ± 7.44 | <0.001 |
| LAV/height2 (mL/m2) | 14.02 ± 4.30 | 18.25 ± 4.96 | <0.001 |
BMI, body mass index; BSA, body surface area; BSA, body surface area; DBP, diastolic blood pressure; HR, heart rate; IVSTd, interventricular septum thickness at end-diastole; LAV, left atrial volume; LVEDD, left ventricular end-diastolic diameter; LVEF, left ventricular ejection fraction; LVM, left ventricular mass; LVPWTd, left ventricular posterior wall thickness at end-diastole; RWT, relative wall thickness; SBP, systolic blood pressure; SD, standard deviation.
Baseline characteristics and echocardiographic measurements in healthy volunteers selected from the EMINCA study population and hypertensive patients (mean ± SD)
| Healthy volunteers (n = 612) | Hypertensive patients (n = 306) | P-value | |
|---|---|---|---|
| Age (years) | 57.07 ± 10.80 | 56.95 ± 10.19 | 0.874 |
| Sex, male | 332 (54.2%) | 181 (59.2%) | 0.159 |
| Height (cm) | 166.13 ± 8.19 | 166.22 ± 7.62 | 0.874 |
| Weight (kg) | 64.59 ± 9.35 | 73.10 ± 12.87 | <0.001 |
| BMI (kg/m2) | 23.31 ± 2.09 | 26.36 ± 3.67 | <0.001 |
| BSA (m2) | 1.75 ± 0.16 | 1.81 ± 0.18 | <0.001 |
| SBP (mmHg) | 120.65 ± 9.82 | 146.87 ± 17.43 | <0.001 |
| DBP (mmHg) | 76.43 ± 7.10 | 87.18 ± 12.82 | <0.001 |
| HR (bpm) | 71.98 ± 8.33 | 71.72 ± 11.34 | 0.725 |
| IVSTd (mm) | 8.88 ± 1.32 | 11.44 ± 1.62 | <0.001 |
| LVEDD (mm) | 45.04 ± 4.06 | 45.36 ± 4.28 | 0.270 |
| LVEDD/BSA (mm/m2) | 25.92 ± 2.63 | 25.21 ± 2.62 | <0.001 |
| LVPWTd (mm) | 8.59 ± 1.25 | 10.11 ± 1.37 | <0.001 |
| RWT | 0.38 ± 0.06 | 0.45 ± 0.07 | <0.001 |
| LVM (g) | 129.65 ± 32.23 | 174.73 ± 42.45 | <0.001 |
| LVM/BSA (g/m2) | 74.21 ± 17.02 | 96.36 ± 20.23 | <0.001 |
| LVM/height2.7 (g/m2.7) | 32.99 ± 7.95 | 44.20 ± 9.67 | <0.001 |
| LVM/height1.7 (g/m1.7) | 54.67 ± 12.83 | 73.41 ± 16.18 | <0.001 |
| LVEF (%) | 65.12 ± 6.02 | 65.75 ± 6.55 | 0.153 |
| LAV (mL) | 38.43 ± 11.49 | 50.09 ± 13.10 | <0.001 |
| LAV/BSA (mL/m2) | 22.11 ± 6.61 | 27.87 ± 7.44 | <0.001 |
| LAV/height2 (mL/m2) | 14.02 ± 4.30 | 18.25 ± 4.96 | <0.001 |
| Healthy volunteers (n = 612) | Hypertensive patients (n = 306) | P-value | |
|---|---|---|---|
| Age (years) | 57.07 ± 10.80 | 56.95 ± 10.19 | 0.874 |
| Sex, male | 332 (54.2%) | 181 (59.2%) | 0.159 |
| Height (cm) | 166.13 ± 8.19 | 166.22 ± 7.62 | 0.874 |
| Weight (kg) | 64.59 ± 9.35 | 73.10 ± 12.87 | <0.001 |
| BMI (kg/m2) | 23.31 ± 2.09 | 26.36 ± 3.67 | <0.001 |
| BSA (m2) | 1.75 ± 0.16 | 1.81 ± 0.18 | <0.001 |
| SBP (mmHg) | 120.65 ± 9.82 | 146.87 ± 17.43 | <0.001 |
| DBP (mmHg) | 76.43 ± 7.10 | 87.18 ± 12.82 | <0.001 |
| HR (bpm) | 71.98 ± 8.33 | 71.72 ± 11.34 | 0.725 |
| IVSTd (mm) | 8.88 ± 1.32 | 11.44 ± 1.62 | <0.001 |
| LVEDD (mm) | 45.04 ± 4.06 | 45.36 ± 4.28 | 0.270 |
| LVEDD/BSA (mm/m2) | 25.92 ± 2.63 | 25.21 ± 2.62 | <0.001 |
| LVPWTd (mm) | 8.59 ± 1.25 | 10.11 ± 1.37 | <0.001 |
| RWT | 0.38 ± 0.06 | 0.45 ± 0.07 | <0.001 |
| LVM (g) | 129.65 ± 32.23 | 174.73 ± 42.45 | <0.001 |
| LVM/BSA (g/m2) | 74.21 ± 17.02 | 96.36 ± 20.23 | <0.001 |
| LVM/height2.7 (g/m2.7) | 32.99 ± 7.95 | 44.20 ± 9.67 | <0.001 |
| LVM/height1.7 (g/m1.7) | 54.67 ± 12.83 | 73.41 ± 16.18 | <0.001 |
| LVEF (%) | 65.12 ± 6.02 | 65.75 ± 6.55 | 0.153 |
| LAV (mL) | 38.43 ± 11.49 | 50.09 ± 13.10 | <0.001 |
| LAV/BSA (mL/m2) | 22.11 ± 6.61 | 27.87 ± 7.44 | <0.001 |
| LAV/height2 (mL/m2) | 14.02 ± 4.30 | 18.25 ± 4.96 | <0.001 |
BMI, body mass index; BSA, body surface area; BSA, body surface area; DBP, diastolic blood pressure; HR, heart rate; IVSTd, interventricular septum thickness at end-diastole; LAV, left atrial volume; LVEDD, left ventricular end-diastolic diameter; LVEF, left ventricular ejection fraction; LVM, left ventricular mass; LVPWTd, left ventricular posterior wall thickness at end-diastole; RWT, relative wall thickness; SBP, systolic blood pressure; SD, standard deviation.
The gender difference in baseline characteristics of the two groups is shown in Table 2. In the healthy volunteer group, age, LVEDD/BSA, LAV/BSA, and LAV/H2 were higher, whereas height, weight, BMI, BSA, SBP, DBP, IVSTd, LVEDD, LVPWTd, LVM, LVM/BSA, and LVM/H1.7 were lower in women than men. In the hypertensive patient group, age, SBP, LVEDD/BSA, LAV/BSA, and LAV/H2 were higher, whereas height, body weight, BSA, IVSTd, LVPWTd, LVEDD, LVM, and LVM/BSA were lower in women than in men.
Baseline characteristics and echocardiographic measurements in healthy volunteers selected from the EMINCA study population and hypertensive patients stratified by gender (mean ± SD)
| Healthy volunteers (n = 612) | Hypertensive patients (n = 306) | |||
|---|---|---|---|---|
| Men (n = 332) | Women (n = 280) | Men (n = 181) | Women (n = 125) | |
| Age (years) | 54.38 ± 10.79 | 60.26 ± 9.93** | 55.56 ± 10.62 | 58.98 ± 9.21## |
| Height (cm) | 171.60 ± 5.61 | 159.60 ± 5.61** | 171.07 ± 4.93 | 159.20 ± 4.84## |
| Weight (kg) | 69.81 ± 7.68 | 58.36 ± 7.01** | 77.87 ± 12.24 | 66.19 ± 10.41## |
| BMI (kg/m2) | 23.67 ± 1.94 | 22.88 ± 2.12** | 26.56 ± 3.65 | 26.07 ± 3.68 |
| BSA (m2) | 1.85 ± 0.13 | 1.63 ± 0.12** | 1.90 ± 0.15 | 1.68 ± 0.13## |
| SBP (mmHg) | 121.49 ± 9.47 | 119.67 ± 10.14* | 144.78 ± 18.44 | 149.90 ± 15.43# |
| DBP (mmHg) | 77.08 ± 6.59 | 75.67 ± 7.59* | 87.76 ± 13.70 | 86.34 ± 11.44 |
| HR (bpm) | 71.54 ± 8.39 | 72.51 ± 8.24 | 71.38 ± 11.11 | 72.22 ± 11.71 |
| IVSTd (mm) | 9.09 ± 1.23 | 8.63 ± 1.30** | 11.76 ± 1.59 | 10.97 ± 1.57## |
| LVEDD (mm) | 46.43 ± 4.02 | 43.38 ± 3.46** | 46.19 ± 4.20 | 44.14 ± 4.10## |
| LVEDD/BSA (mm/m2) | 25.18 ± 2.51 | 26.79 ± 2.50** | 24.43 ± 2.40 | 26.35 ± 2.51## |
| LVPWTd (mm) | 8.81 ± 1.27 | 8.33 ± 1.18** | 10.40 ± 1.41 | 9.69 ± 1.20## |
| RWT | 0.38 ± 0.07 | 0.39 ± 0.06 | 0.45 ± 0.08 | 0.44 ± 0.06 |
| LVM (g) | 140.43 ± 32.01 | 116.87 ± 27.52** | 186.55 ± 41.89 | 157.61 ± 37.22## |
| LVM/BSA (g/m2) | 75.99 ± 16.96 | 72.08 ± 16.89** | 98.36 ± 20.83 | 93.46 ± 19.05# |
| LVM/height2.7 (g/m2.7) | 32.77 ± 7.72 | 33.25 ± 8.23 | 43.78 ± 9.72 | 44.80 ± 9.60 |
| LVM/height1.7 (g/m1.7) | 56.13 ± 12.84 | 52.92 ± 12.61** | 74.84 ± 16.44 | 71.33 ± 15.63 |
| LVEF (%) | 64.89 ± 5.89 | 65.40 ± 6.21 | 65.43 ± 6.85 | 66.21 ± 6.09 |
| LAV (mL) | 38.85 ± 11.82 | 37.94 ± 11.10 | 50.73 ± 13.31 | 49.23 ± 12.83 |
| LAV/BSA (mL/m2) | 21.04 ± 6.31 | 23.37 ± 6.74** | 26.66 ± 7.13 | 29.48 ± 7.58## |
| LAV/height2 (mL/m2) | 13.23 ± 4.08 | 14.93 ± 4.37** | 17.32 ± 4.62 | 19.49 ± 5.15## |
| Healthy volunteers (n = 612) | Hypertensive patients (n = 306) | |||
|---|---|---|---|---|
| Men (n = 332) | Women (n = 280) | Men (n = 181) | Women (n = 125) | |
| Age (years) | 54.38 ± 10.79 | 60.26 ± 9.93** | 55.56 ± 10.62 | 58.98 ± 9.21## |
| Height (cm) | 171.60 ± 5.61 | 159.60 ± 5.61** | 171.07 ± 4.93 | 159.20 ± 4.84## |
| Weight (kg) | 69.81 ± 7.68 | 58.36 ± 7.01** | 77.87 ± 12.24 | 66.19 ± 10.41## |
| BMI (kg/m2) | 23.67 ± 1.94 | 22.88 ± 2.12** | 26.56 ± 3.65 | 26.07 ± 3.68 |
| BSA (m2) | 1.85 ± 0.13 | 1.63 ± 0.12** | 1.90 ± 0.15 | 1.68 ± 0.13## |
| SBP (mmHg) | 121.49 ± 9.47 | 119.67 ± 10.14* | 144.78 ± 18.44 | 149.90 ± 15.43# |
| DBP (mmHg) | 77.08 ± 6.59 | 75.67 ± 7.59* | 87.76 ± 13.70 | 86.34 ± 11.44 |
| HR (bpm) | 71.54 ± 8.39 | 72.51 ± 8.24 | 71.38 ± 11.11 | 72.22 ± 11.71 |
| IVSTd (mm) | 9.09 ± 1.23 | 8.63 ± 1.30** | 11.76 ± 1.59 | 10.97 ± 1.57## |
| LVEDD (mm) | 46.43 ± 4.02 | 43.38 ± 3.46** | 46.19 ± 4.20 | 44.14 ± 4.10## |
| LVEDD/BSA (mm/m2) | 25.18 ± 2.51 | 26.79 ± 2.50** | 24.43 ± 2.40 | 26.35 ± 2.51## |
| LVPWTd (mm) | 8.81 ± 1.27 | 8.33 ± 1.18** | 10.40 ± 1.41 | 9.69 ± 1.20## |
| RWT | 0.38 ± 0.07 | 0.39 ± 0.06 | 0.45 ± 0.08 | 0.44 ± 0.06 |
| LVM (g) | 140.43 ± 32.01 | 116.87 ± 27.52** | 186.55 ± 41.89 | 157.61 ± 37.22## |
| LVM/BSA (g/m2) | 75.99 ± 16.96 | 72.08 ± 16.89** | 98.36 ± 20.83 | 93.46 ± 19.05# |
| LVM/height2.7 (g/m2.7) | 32.77 ± 7.72 | 33.25 ± 8.23 | 43.78 ± 9.72 | 44.80 ± 9.60 |
| LVM/height1.7 (g/m1.7) | 56.13 ± 12.84 | 52.92 ± 12.61** | 74.84 ± 16.44 | 71.33 ± 15.63 |
| LVEF (%) | 64.89 ± 5.89 | 65.40 ± 6.21 | 65.43 ± 6.85 | 66.21 ± 6.09 |
| LAV (mL) | 38.85 ± 11.82 | 37.94 ± 11.10 | 50.73 ± 13.31 | 49.23 ± 12.83 |
| LAV/BSA (mL/m2) | 21.04 ± 6.31 | 23.37 ± 6.74** | 26.66 ± 7.13 | 29.48 ± 7.58## |
| LAV/height2 (mL/m2) | 13.23 ± 4.08 | 14.93 ± 4.37** | 17.32 ± 4.62 | 19.49 ± 5.15## |
BMI, body mass index; BSA, body surface area; BSA, body surface area; DBP, diastolic blood pressure; HR, heart rate; IVSTd, interventricular septum thickness at end-diastole; LAV, left atrial volume; LVEDD, left ventricular end-diastolic diameter; LVEF, left ventricular ejection fraction; LVM, left ventricular mass; LVPWTd, left ventricular posterior wall thickness at end-diastole; RWT, relative wall thickness; SBP, systolic blood pressure; SD, standard deviation.
P < 0.05,
P < 0.01, vs. men of healthy volunteers;
P < 0.05,
P < 0.01, vs. men of hypertensive patients.
Baseline characteristics and echocardiographic measurements in healthy volunteers selected from the EMINCA study population and hypertensive patients stratified by gender (mean ± SD)
| Healthy volunteers (n = 612) | Hypertensive patients (n = 306) | |||
|---|---|---|---|---|
| Men (n = 332) | Women (n = 280) | Men (n = 181) | Women (n = 125) | |
| Age (years) | 54.38 ± 10.79 | 60.26 ± 9.93** | 55.56 ± 10.62 | 58.98 ± 9.21## |
| Height (cm) | 171.60 ± 5.61 | 159.60 ± 5.61** | 171.07 ± 4.93 | 159.20 ± 4.84## |
| Weight (kg) | 69.81 ± 7.68 | 58.36 ± 7.01** | 77.87 ± 12.24 | 66.19 ± 10.41## |
| BMI (kg/m2) | 23.67 ± 1.94 | 22.88 ± 2.12** | 26.56 ± 3.65 | 26.07 ± 3.68 |
| BSA (m2) | 1.85 ± 0.13 | 1.63 ± 0.12** | 1.90 ± 0.15 | 1.68 ± 0.13## |
| SBP (mmHg) | 121.49 ± 9.47 | 119.67 ± 10.14* | 144.78 ± 18.44 | 149.90 ± 15.43# |
| DBP (mmHg) | 77.08 ± 6.59 | 75.67 ± 7.59* | 87.76 ± 13.70 | 86.34 ± 11.44 |
| HR (bpm) | 71.54 ± 8.39 | 72.51 ± 8.24 | 71.38 ± 11.11 | 72.22 ± 11.71 |
| IVSTd (mm) | 9.09 ± 1.23 | 8.63 ± 1.30** | 11.76 ± 1.59 | 10.97 ± 1.57## |
| LVEDD (mm) | 46.43 ± 4.02 | 43.38 ± 3.46** | 46.19 ± 4.20 | 44.14 ± 4.10## |
| LVEDD/BSA (mm/m2) | 25.18 ± 2.51 | 26.79 ± 2.50** | 24.43 ± 2.40 | 26.35 ± 2.51## |
| LVPWTd (mm) | 8.81 ± 1.27 | 8.33 ± 1.18** | 10.40 ± 1.41 | 9.69 ± 1.20## |
| RWT | 0.38 ± 0.07 | 0.39 ± 0.06 | 0.45 ± 0.08 | 0.44 ± 0.06 |
| LVM (g) | 140.43 ± 32.01 | 116.87 ± 27.52** | 186.55 ± 41.89 | 157.61 ± 37.22## |
| LVM/BSA (g/m2) | 75.99 ± 16.96 | 72.08 ± 16.89** | 98.36 ± 20.83 | 93.46 ± 19.05# |
| LVM/height2.7 (g/m2.7) | 32.77 ± 7.72 | 33.25 ± 8.23 | 43.78 ± 9.72 | 44.80 ± 9.60 |
| LVM/height1.7 (g/m1.7) | 56.13 ± 12.84 | 52.92 ± 12.61** | 74.84 ± 16.44 | 71.33 ± 15.63 |
| LVEF (%) | 64.89 ± 5.89 | 65.40 ± 6.21 | 65.43 ± 6.85 | 66.21 ± 6.09 |
| LAV (mL) | 38.85 ± 11.82 | 37.94 ± 11.10 | 50.73 ± 13.31 | 49.23 ± 12.83 |
| LAV/BSA (mL/m2) | 21.04 ± 6.31 | 23.37 ± 6.74** | 26.66 ± 7.13 | 29.48 ± 7.58## |
| LAV/height2 (mL/m2) | 13.23 ± 4.08 | 14.93 ± 4.37** | 17.32 ± 4.62 | 19.49 ± 5.15## |
| Healthy volunteers (n = 612) | Hypertensive patients (n = 306) | |||
|---|---|---|---|---|
| Men (n = 332) | Women (n = 280) | Men (n = 181) | Women (n = 125) | |
| Age (years) | 54.38 ± 10.79 | 60.26 ± 9.93** | 55.56 ± 10.62 | 58.98 ± 9.21## |
| Height (cm) | 171.60 ± 5.61 | 159.60 ± 5.61** | 171.07 ± 4.93 | 159.20 ± 4.84## |
| Weight (kg) | 69.81 ± 7.68 | 58.36 ± 7.01** | 77.87 ± 12.24 | 66.19 ± 10.41## |
| BMI (kg/m2) | 23.67 ± 1.94 | 22.88 ± 2.12** | 26.56 ± 3.65 | 26.07 ± 3.68 |
| BSA (m2) | 1.85 ± 0.13 | 1.63 ± 0.12** | 1.90 ± 0.15 | 1.68 ± 0.13## |
| SBP (mmHg) | 121.49 ± 9.47 | 119.67 ± 10.14* | 144.78 ± 18.44 | 149.90 ± 15.43# |
| DBP (mmHg) | 77.08 ± 6.59 | 75.67 ± 7.59* | 87.76 ± 13.70 | 86.34 ± 11.44 |
| HR (bpm) | 71.54 ± 8.39 | 72.51 ± 8.24 | 71.38 ± 11.11 | 72.22 ± 11.71 |
| IVSTd (mm) | 9.09 ± 1.23 | 8.63 ± 1.30** | 11.76 ± 1.59 | 10.97 ± 1.57## |
| LVEDD (mm) | 46.43 ± 4.02 | 43.38 ± 3.46** | 46.19 ± 4.20 | 44.14 ± 4.10## |
| LVEDD/BSA (mm/m2) | 25.18 ± 2.51 | 26.79 ± 2.50** | 24.43 ± 2.40 | 26.35 ± 2.51## |
| LVPWTd (mm) | 8.81 ± 1.27 | 8.33 ± 1.18** | 10.40 ± 1.41 | 9.69 ± 1.20## |
| RWT | 0.38 ± 0.07 | 0.39 ± 0.06 | 0.45 ± 0.08 | 0.44 ± 0.06 |
| LVM (g) | 140.43 ± 32.01 | 116.87 ± 27.52** | 186.55 ± 41.89 | 157.61 ± 37.22## |
| LVM/BSA (g/m2) | 75.99 ± 16.96 | 72.08 ± 16.89** | 98.36 ± 20.83 | 93.46 ± 19.05# |
| LVM/height2.7 (g/m2.7) | 32.77 ± 7.72 | 33.25 ± 8.23 | 43.78 ± 9.72 | 44.80 ± 9.60 |
| LVM/height1.7 (g/m1.7) | 56.13 ± 12.84 | 52.92 ± 12.61** | 74.84 ± 16.44 | 71.33 ± 15.63 |
| LVEF (%) | 64.89 ± 5.89 | 65.40 ± 6.21 | 65.43 ± 6.85 | 66.21 ± 6.09 |
| LAV (mL) | 38.85 ± 11.82 | 37.94 ± 11.10 | 50.73 ± 13.31 | 49.23 ± 12.83 |
| LAV/BSA (mL/m2) | 21.04 ± 6.31 | 23.37 ± 6.74** | 26.66 ± 7.13 | 29.48 ± 7.58## |
| LAV/height2 (mL/m2) | 13.23 ± 4.08 | 14.93 ± 4.37** | 17.32 ± 4.62 | 19.49 ± 5.15## |
BMI, body mass index; BSA, body surface area; BSA, body surface area; DBP, diastolic blood pressure; HR, heart rate; IVSTd, interventricular septum thickness at end-diastole; LAV, left atrial volume; LVEDD, left ventricular end-diastolic diameter; LVEF, left ventricular ejection fraction; LVM, left ventricular mass; LVPWTd, left ventricular posterior wall thickness at end-diastole; RWT, relative wall thickness; SBP, systolic blood pressure; SD, standard deviation.
P < 0.05,
P < 0.01, vs. men of healthy volunteers;
P < 0.05,
P < 0.01, vs. men of hypertensive patients.
Thresholds for LV and LA parameters according to guidelines and from selected subjects in EMINCA study
According to the ASE/EACVI and ESC/ESH guidelines,11,12,17 when indexed to BSA (LVM/BSA), the upper normal limit or threshold for LVM index (LVMI) was >115 g/m2 in men and >95 g/m2 in women, and when indexed to height2.7 (LVM/H2.7), the threshold for LVMI was >50 g/H2.7 in men and >47 g/H2.7 in women. According to Chirinos et al.,18 when indexed to height1.7 (LVM/H1.7), the threshold for LVMI was >81 g/H1.7 in men and >60 g/H1.7 in women. The threshold for RWT was >0.42 for both sexes without indexing.11,12 When indexed to BSA (LAV/BSA), the threshold for LA volume index (LAVI) was >34 mL/m2 for both men and women.12 According to the ESC/ESH guidelines, when indexed to height2 (LAV/H2), the threshold for LAVI was >18.5 mL/H2 in men and >16.5 mL/H2 in women17 (Table 3).
Normal reference values of echocardiographic measurements from healthy volunteers selected from the EMINCA population and international guidelines and Chirinos et al (95% CI)
| Healthy volunteers | Guidelines and Chirinos et al. | |||
|---|---|---|---|---|
| Men | Women | Men | Women | |
| IVSTd (mm)a,b | 7–12 | 6–11 | 6–10 | 6–9 |
| LVEDD (mm)b | 39–54 | 37–50 | 42–58 | 38–52 |
| LVEDD/BSA (mm/m2)b | 20–30 | 22–32 | 22–30 | 23–31 |
| LVPWTd (mm)a,b | 6–11 | 6–11 | 6–10 | 6–9 |
| RWT (cm)a,b | 0.25–0.51 | 0.27–0.51 | 0.24–0.42 | 0.22–0.42 |
| LVM (g)a,b | 78–203 | 63–171 | 88–224 | 67–162 |
| LVM/BSA (g/m2)a,b | 43–109 | 39–105 | 49–115 | 43–95 |
| LVM/height2.7 (g/m2.7)c | 18–48 | 17–49 | NA–50 | NA–47 |
| LVM/height1.7 (g/m1.7)d | 31–81 | 28–78 | 41–81 | 33–60 |
| LAV/BSA (mL/m2)b | 9–33 | 10–37 | 16–34 | 16–34 |
| LAV/height2 (mL/m2)c | 5–21.2 | 6–23.5 | NA–18.5 | NA–16.5 |
| Healthy volunteers | Guidelines and Chirinos et al. | |||
|---|---|---|---|---|
| Men | Women | Men | Women | |
| IVSTd (mm)a,b | 7–12 | 6–11 | 6–10 | 6–9 |
| LVEDD (mm)b | 39–54 | 37–50 | 42–58 | 38–52 |
| LVEDD/BSA (mm/m2)b | 20–30 | 22–32 | 22–30 | 23–31 |
| LVPWTd (mm)a,b | 6–11 | 6–11 | 6–10 | 6–9 |
| RWT (cm)a,b | 0.25–0.51 | 0.27–0.51 | 0.24–0.42 | 0.22–0.42 |
| LVM (g)a,b | 78–203 | 63–171 | 88–224 | 67–162 |
| LVM/BSA (g/m2)a,b | 43–109 | 39–105 | 49–115 | 43–95 |
| LVM/height2.7 (g/m2.7)c | 18–48 | 17–49 | NA–50 | NA–47 |
| LVM/height1.7 (g/m1.7)d | 31–81 | 28–78 | 41–81 | 33–60 |
| LAV/BSA (mL/m2)b | 9–33 | 10–37 | 16–34 | 16–34 |
| LAV/height2 (mL/m2)c | 5–21.2 | 6–23.5 | NA–18.5 | NA–16.5 |
BSA, body surface area; CI, confidence interval; IVSTd, interventricular septum thickness at end-diastole; LAV, left atrial volume; LVEDD, left ventricular end-diastolic diameter; LVM, left ventricular mass; LVPWTd, left ventricular posterior wall thickness at end-diastole; NA, not available; RWT, relative wall thickness.
Guideline thresholds from recommendations on the use of echocardiography in adult hypertension: a report from the European Association of Cardiovascular Imaging (EACVI) and the American Society of Echocardiography (ASE).11
Guideline thresholds from recommendations for cardiac chamber quantification by echocardiography in adults: an update from the ASE and EACVI.12
Guideline thresholds from 2018 ESC/ESH guidelines for the management of arterial hypertension.17
Thresholds defined by Chirinos et al.18
Normal reference values of echocardiographic measurements from healthy volunteers selected from the EMINCA population and international guidelines and Chirinos et al (95% CI)
| Healthy volunteers | Guidelines and Chirinos et al. | |||
|---|---|---|---|---|
| Men | Women | Men | Women | |
| IVSTd (mm)a,b | 7–12 | 6–11 | 6–10 | 6–9 |
| LVEDD (mm)b | 39–54 | 37–50 | 42–58 | 38–52 |
| LVEDD/BSA (mm/m2)b | 20–30 | 22–32 | 22–30 | 23–31 |
| LVPWTd (mm)a,b | 6–11 | 6–11 | 6–10 | 6–9 |
| RWT (cm)a,b | 0.25–0.51 | 0.27–0.51 | 0.24–0.42 | 0.22–0.42 |
| LVM (g)a,b | 78–203 | 63–171 | 88–224 | 67–162 |
| LVM/BSA (g/m2)a,b | 43–109 | 39–105 | 49–115 | 43–95 |
| LVM/height2.7 (g/m2.7)c | 18–48 | 17–49 | NA–50 | NA–47 |
| LVM/height1.7 (g/m1.7)d | 31–81 | 28–78 | 41–81 | 33–60 |
| LAV/BSA (mL/m2)b | 9–33 | 10–37 | 16–34 | 16–34 |
| LAV/height2 (mL/m2)c | 5–21.2 | 6–23.5 | NA–18.5 | NA–16.5 |
| Healthy volunteers | Guidelines and Chirinos et al. | |||
|---|---|---|---|---|
| Men | Women | Men | Women | |
| IVSTd (mm)a,b | 7–12 | 6–11 | 6–10 | 6–9 |
| LVEDD (mm)b | 39–54 | 37–50 | 42–58 | 38–52 |
| LVEDD/BSA (mm/m2)b | 20–30 | 22–32 | 22–30 | 23–31 |
| LVPWTd (mm)a,b | 6–11 | 6–11 | 6–10 | 6–9 |
| RWT (cm)a,b | 0.25–0.51 | 0.27–0.51 | 0.24–0.42 | 0.22–0.42 |
| LVM (g)a,b | 78–203 | 63–171 | 88–224 | 67–162 |
| LVM/BSA (g/m2)a,b | 43–109 | 39–105 | 49–115 | 43–95 |
| LVM/height2.7 (g/m2.7)c | 18–48 | 17–49 | NA–50 | NA–47 |
| LVM/height1.7 (g/m1.7)d | 31–81 | 28–78 | 41–81 | 33–60 |
| LAV/BSA (mL/m2)b | 9–33 | 10–37 | 16–34 | 16–34 |
| LAV/height2 (mL/m2)c | 5–21.2 | 6–23.5 | NA–18.5 | NA–16.5 |
BSA, body surface area; CI, confidence interval; IVSTd, interventricular septum thickness at end-diastole; LAV, left atrial volume; LVEDD, left ventricular end-diastolic diameter; LVM, left ventricular mass; LVPWTd, left ventricular posterior wall thickness at end-diastole; NA, not available; RWT, relative wall thickness.
Guideline thresholds from recommendations on the use of echocardiography in adult hypertension: a report from the European Association of Cardiovascular Imaging (EACVI) and the American Society of Echocardiography (ASE).11
Guideline thresholds from recommendations for cardiac chamber quantification by echocardiography in adults: an update from the ASE and EACVI.12
Guideline thresholds from 2018 ESC/ESH guidelines for the management of arterial hypertension.17
Thresholds defined by Chirinos et al.18
The normal echocardiographic reference values measured in the healthy volunteer group are listed in Table 3. Compared with the values recommended by ASE/EACVI and ESC/ESH,11,12,17 the upper limits of IVSTd, LVPWTd, RWT, and LAV/height2 were higher, whereas those of LVEDD were smaller in both genders of the Chinese healthy volunteer group, although the difference in LVEDD disappeared after indexation to BSA. When indexed to BSA (LVM/BSA), the threshold for LVMI was >109 g/m2 in men and >105 g/m2 in women. When indexed to height2.7 (LVM/H2.7), the threshold for LVMI was >48 g/H2.7 in men and >49 g/H2.7 in women. When indexed to height1.7 (LVM/H1.7), the threshold for LVMI was >81 g/H1.7 in men and >78 g/H1.7 in women. The threshold for RWT was >0.51 in both men and women, which was much higher than the RWT recommended by the ASE/EACVI guidelines (Table 3). When indexed to BSA (LAV/BSA), the threshold for LAVI was >33 mL/m2 in men and >37 mL/m2 in women. When indexed to H2 (LAV/H2), the threshold for LAVI was >21.2 mL/H2 in men and >23.5 mL/H2 in women.
The prevalence of LVH, defined as LVMI larger than the thresholds from the guidelines and the healthy volunteer group, is compared in Figure 2A. When LVM was indexed to BSA or H2.7, the prevalence of LVH showed no significant difference using thresholds from the guidelines11,12,17 and the healthy volunteer group. However, when LVM was indexed to H1.7, the prevalence of LVH was significantly higher using thresholds from Chirinos et al.18 than from the healthy volunteer group, likely due to a much lower threshold from the former than the latter in women (Table 3).
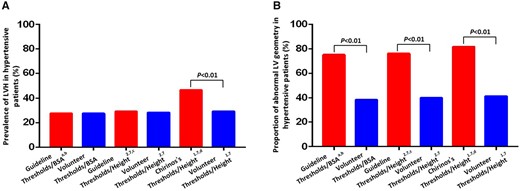
Prevalence of LVH (A) and the total proportion of abnormal LV geometric patterns (B) in hypertensive patients using different thresholds and indexing methods. BSA, body surface area; LV, left ventricular; LVH, left ventricular hypertrophy. aThresholds from recommendations on the use of echocardiography in adult hypertension: a report from the European Association of Cardiovascular Imaging (EACVI) and the American Society of Echocardiography (ASE).11 bThresholds from recommendations for cardiac chamber quantification by echocardiography in adults: an update from the ASE and EACVI.12 cThresholds from 2018 ESC/ESH guidelines for the management of arterial hypertension.17 dThresholds from Chirinos’s et al.18
LV geometric patterns in hypertensive patients using thresholds from guidelines and the healthy volunteer group
The proportion of the four LV geometry patterns in hypertensive patients based on thresholds from guidelines and the healthy volunteer group using indexation to BSA, H2.7, or H1.7 is shown in Table 4. When LVM was indexed to BSA, the proportion of concentric remodelling was the largest, followed by normal geometry, concentric hypertrophy, and eccentric hypertrophy, when using thresholds from guidelines.11,12 In contrast, the proportion of normal geometry was the highest, followed by eccentric hypertrophy, concentric remodelling, and concentric hypertrophy, when using thresholds from the healthy volunteer group. As a result, the proportions of normal geometry and eccentric hypertrophy were substantially higher (P < 0.01), while those of concentric remodelling and concentric hypertrophy were lower (P < 0.01) using thresholds from the healthy volunteer group than using thresholds from guidelines. Similarly, when LVM was indexed to H2.7 or H1.7, the proportions of normal geometry and eccentric hypertrophy were higher while those of concentric remodelling and concentric hypertrophy were lower using thresholds from the healthy volunteer group than using thresholds from guidelines17 or Chirinos et al.18 We further calculated the total proportion of abnormal LV geometric patterns (eccentric hypertrophy, concentric remodelling, and concentric hypertrophy) and found that these abnormal patterns were significantly lower when using thresholds from the healthy volunteer group than when using thresholds from guidelines, whether LVM was indexed to BSA, H2.7, or H1.7 (P < 0.01) (Figure 2B). A major reason for such a difference was a much lower proportion of concentric remodelling using the healthy volunteer group-defined thresholds than using guideline-defined thresholds. It was also evident from Figure 2A and B that the total proportion of abnormal LV geometric patterns was higher than the prevalence of LVH when using the healthy volunteer group- and guideline-defined thresholds and when LVM was indexed to BSA, H2.7, and H1.7 in hypertensive patients. This suggests that abnormal LV geometric patterns were more sensitive to reflect LV remodelling in hypertensive patients than LV hypertrophy alone.
LV geometric patterns in hypertensive patients using different thresholds and indexation methods (cases, %)
| NG | CR | EH | CH | |
|---|---|---|---|---|
| Guideline thresholds/BSA | 76 (24.8%) | 146 (47.7%) | 26 (8.5%) | 58 (19.0%) |
| Volunteer thresholds/BSA | 189 (61.8%)** | 33 (10.8%)** | 65 (21.2%)** | 19 (6.2%)** |
| Guideline thresholds/height2.7 | 73 (23.8%) | 144 (47.1%) | 29 (9.5%) | 60 (19.6%) |
| Volunteer thresholds/height2.7 | 184 (60.1%)## | 36 (11.8%)## | 70 (22.9%)## | 16 (5.2%)## |
| Chirinos’s thresholds/height1.7 | 56 (18.3%) | 108 (35.3%) | 46 (15.0%) | 96 (31.4%) |
| Volunteer thresholds/height1.7 | 180 (58.8%)†† | 37 (12.1%)†† | 74 (24.2%)†† | 15 (4.9%)†† |
| NG | CR | EH | CH | |
|---|---|---|---|---|
| Guideline thresholds/BSA | 76 (24.8%) | 146 (47.7%) | 26 (8.5%) | 58 (19.0%) |
| Volunteer thresholds/BSA | 189 (61.8%)** | 33 (10.8%)** | 65 (21.2%)** | 19 (6.2%)** |
| Guideline thresholds/height2.7 | 73 (23.8%) | 144 (47.1%) | 29 (9.5%) | 60 (19.6%) |
| Volunteer thresholds/height2.7 | 184 (60.1%)## | 36 (11.8%)## | 70 (22.9%)## | 16 (5.2%)## |
| Chirinos’s thresholds/height1.7 | 56 (18.3%) | 108 (35.3%) | 46 (15.0%) | 96 (31.4%) |
| Volunteer thresholds/height1.7 | 180 (58.8%)†† | 37 (12.1%)†† | 74 (24.2%)†† | 15 (4.9%)†† |
CH, concentric hypertrophy; CR, concentric remodelling; EH, eccentric hypertrophy; NG, normal geometry.
Vs. Guideline thresholds/BSA, P < 0.01;
vs. Guideline thresholds/height2.7, P < 0.01;
vs. Chirinos’s thresholds/Height1.7, P < 0.01. Volunteer thresholds/BSA, volunteer thresholds/height2.7 and volunteer thresholds/height1.7 represent three different indexation methods for the healthy volunteers selected from the EMINCA study population. Guideline thresholds/BSA and Guideline thresholds/height2.7 represent two different indexation methods recommended by international guidelines. Chirinos’s thresholds/height1.7 represents the indexation method proposed by Chirinos et al.
LV geometric patterns in hypertensive patients using different thresholds and indexation methods (cases, %)
| NG | CR | EH | CH | |
|---|---|---|---|---|
| Guideline thresholds/BSA | 76 (24.8%) | 146 (47.7%) | 26 (8.5%) | 58 (19.0%) |
| Volunteer thresholds/BSA | 189 (61.8%)** | 33 (10.8%)** | 65 (21.2%)** | 19 (6.2%)** |
| Guideline thresholds/height2.7 | 73 (23.8%) | 144 (47.1%) | 29 (9.5%) | 60 (19.6%) |
| Volunteer thresholds/height2.7 | 184 (60.1%)## | 36 (11.8%)## | 70 (22.9%)## | 16 (5.2%)## |
| Chirinos’s thresholds/height1.7 | 56 (18.3%) | 108 (35.3%) | 46 (15.0%) | 96 (31.4%) |
| Volunteer thresholds/height1.7 | 180 (58.8%)†† | 37 (12.1%)†† | 74 (24.2%)†† | 15 (4.9%)†† |
| NG | CR | EH | CH | |
|---|---|---|---|---|
| Guideline thresholds/BSA | 76 (24.8%) | 146 (47.7%) | 26 (8.5%) | 58 (19.0%) |
| Volunteer thresholds/BSA | 189 (61.8%)** | 33 (10.8%)** | 65 (21.2%)** | 19 (6.2%)** |
| Guideline thresholds/height2.7 | 73 (23.8%) | 144 (47.1%) | 29 (9.5%) | 60 (19.6%) |
| Volunteer thresholds/height2.7 | 184 (60.1%)## | 36 (11.8%)## | 70 (22.9%)## | 16 (5.2%)## |
| Chirinos’s thresholds/height1.7 | 56 (18.3%) | 108 (35.3%) | 46 (15.0%) | 96 (31.4%) |
| Volunteer thresholds/height1.7 | 180 (58.8%)†† | 37 (12.1%)†† | 74 (24.2%)†† | 15 (4.9%)†† |
CH, concentric hypertrophy; CR, concentric remodelling; EH, eccentric hypertrophy; NG, normal geometry.
Vs. Guideline thresholds/BSA, P < 0.01;
vs. Guideline thresholds/height2.7, P < 0.01;
vs. Chirinos’s thresholds/Height1.7, P < 0.01. Volunteer thresholds/BSA, volunteer thresholds/height2.7 and volunteer thresholds/height1.7 represent three different indexation methods for the healthy volunteers selected from the EMINCA study population. Guideline thresholds/BSA and Guideline thresholds/height2.7 represent two different indexation methods recommended by international guidelines. Chirinos’s thresholds/height1.7 represents the indexation method proposed by Chirinos et al.
LA dilation in hypertensive patients using thresholds from guidelines and the healthy volunteer group
The prevalence of LA dilatation defined as LAVI larger than thresholds defined by guidelines12,17 and from the healthy volunteer group was compared in Figure 3. When LAV was indexed to BSA, the prevalence of LA dilatation showed no significant difference using thresholds either from the guidelines12 or the healthy volunteer group. In contrast, when LAV was indexed to H2, the prevalence of LA dilatation was significantly lower using thresholds from the healthy volunteer group than using thresholds from guidelines17 (P < 0.01), possibly due to a higher threshold for LAV/H2 in both sexes in the healthy volunteer group.
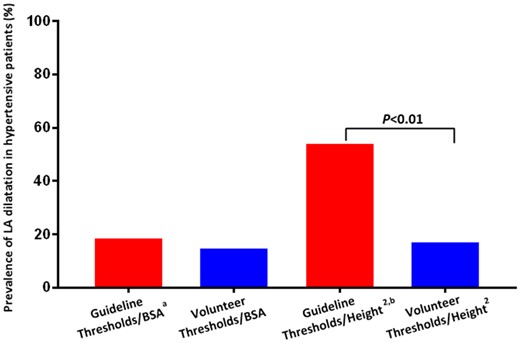
Prevalence of LA dilatation in hypertensive patients using different thresholds and indexing methods. BSA, body surface area; LA, left atrial. aThresholds from recommendations for cardiac chamber quantification by echocardiography in adults: an update from the ASE and EACVI.12 bThresholds from 2018 ESC/ESH Guidelines for the management of arterial hypertension.17
Reproducibility
The intraclass correlation coefficients of intraobserver reproducibility for IVSTd, LVEDD, LVPWTd, and LAV were 0.91, 0.93, 0.95, and 0.97, respectively (P < 0.001 for all). The intraclass correlation coefficients for interobserver reproducibility for IVSTd, LVEDD, LVPWTd, and LAV were 0.92, 0.92, 0.90, and 0.96, respectively (P < 0.001 for all) (Supplementary data online, Figure S1).
Discussion
There were several important findings in this study. First, there was a remarkable difference in echocardiographic thresholds defined by international guidelines and the Chinese healthy volunteers, particularly for LVM indexed to BSA and LAV indexed to H2. Second, when LAV was indexed to H2, the prevalence of LA dilatation was significantly lower in hypertensive patients using thresholds from the healthy volunteer group than using thresholds from guidelines. Third, the proportion of normal geometry and eccentric hypertrophy was substantially higher, while that of concentric remodelling and concentric hypertrophy was lower using thresholds from the healthy volunteer group than using thresholds from guidelines and Chirinos et al. Finally, the total proportion of abnormal LV geometric patterns was significantly lower using thresholds from the healthy volunteer group than using thresholds from guidelines and Chirinos et al. when LVM was indexed to BSA, H2.7, and H1.7. To the best of our knowledge, our study is the first to report the difference in LV and LA remodelling patterns in hypertensive patients using different thresholds defined by international guidelines and the Chinese healthy volunteers and using different indexation methods.
The prerequisite for a correct diagnosis of LV and LA remodelling in hypertensive patients by echocardiography is to distinguish between normal and abnormal values. Current thresholds for discerning LV and LA remodelling recommended by international guidelines are based on normal reference values derived from small samples of Caucasians and are not representative of other ethnic groups such as Chinese individuals. The Echocardiographic Normal Ranges Meta-Analysis of the Left heart (EchoNoRMAL) study found important sex, age, and ethnic differences in LA and ventricular echocardiographic measurements in normal adults even after indexation by BSA or height.19,20 Recent EMINCA and WASE studies also showed that significant differences existed in LV and LA echocardiographic measurements between different nations and ethnic groups14,15; therefore, using thresholds recommended by the ASE/EACVI or ESC/ESH guidelines to detect LV and LA remodelling in non-White hypertensive patients may lead to errors.
Several indexation methods have been recommended by guidelines but none of them is satisfactory. Both EMINCA and WASE studies showed that indexation to BSA or H2.7 cannot completely eliminate the effect of physiological variance on echocardiographic measurements14,15 and may even lead to an overcorrection. This is evident from the higher LAV/BSA and LAV/H2 values in women than men of the healthy volunteer group, and a much lower LAV/H2 values by ESC/ESH guidelines than from the healthy volunteer group (Table 3). Although Chirinos et al.18 demonstrated that indexing LVM to H1.7 was superior to indexing to H2.7 or BSA in predicting cardiovascular events, we still found significant differences in the prevalence of LVH and the proportion of abnormal LV geometric patterns in hypertensive patients using the thresholds by Chirinos et al.18 and from the healthy volunteer group. We recently developed a novel optimized multivariate allometric model for correcting the physiologic variance of echocardiographic measurements, which dramatically increased the success rate of correction.21 Further studies are warranted to establish an accurate indexing algorithm to remove the effect of physiological variance.
In this study, we measured LVMI using techniques and formulas recommended by the ASE/EACVI guidelines.11,12 As shown in Table 3, before indexation, the normal upper thresholds of LVM from the healthy volunteer group were lower than from the guidelines for men, but the opposite occurred for women. The prevalence of LVH in hypertensive patients showed no significant difference using thresholds from the guidelines and the healthy volunteer group, whether LVM was indexed to BSA or H2.7, as shown in Figure 2A. This was because, for both indexation methods, the upper thresholds from the healthy volunteer group were lower than from the guidelines group in men, while the opposite occurred in women, resulting in a similar prevalence of LVH in the whole group using the two indexation methods. However, when LVM was indexed to H1.7, the prevalence of LVH was significantly higher using thresholds from Chirinos et al.18 than from the healthy volunteer group, likely due to a much lower threshold from the former than the latter in women (Table 3).
In patients with hypertension, two basic patterns of LV hypertrophy occur in response to haemodynamic overload. In the first pattern, pressure elevation leads to an increased wall thickness and RWT, a phenomenon known as concentric remodelling. Eventually, an increase in systolic wall stress leads to concentric hypertrophy. In the second pattern, eccentric hypertrophy owing to volume overload is caused by increased diastolic wall stress, thereby engendering LV enlargement. Stress in the wall of the enlarged heart increases with LV size. This increase is compensated by a proportional increase of wall thickness, so that wall stress remains matched with systolic pressure. An important advantage of Ganau’s classification is that it is easy to obtain ventricular wall thickness and LV size in clinical settings to evaluate the type of LV remodelling in hypertension. In this study, we measured RWT using techniques and formulas recommended by the ASE/EACVI guidelines,11,12 and found that RWT values were substantially higher in both sexes derived from the healthy volunteer group than from the guidelines probably due to smaller values of LVEDD and larger values of LVPWTd in the healthy volunteer group. Consequently, thresholds for increased RWT were higher as defined by the healthy volunteer group than by guidelines (Table 3). This explains why the proportion of both concentric remodelling and concentric hypertrophy was lower in hypertensive patients using thresholds from the healthy volunteer group than from guidelines, as these two LV geometric patterns require an increased RWT. In contrast, as both normal geometry and eccentric hypertrophy require a normal RWT, the proportion of these two geometric patterns was markedly higher using thresholds from the healthy volunteer group than from guidelines. Furthermore, the difference in RWT between the healthy volunteer group and guidelines explains why the total proportion of abnormal LV geometric patterns (eccentric hypertrophy, concentric remodelling, and concentric hypertrophy) was significantly lower using thresholds from the healthy volunteer group than from guidelines when LVM was indexed to BSA, H2.7, and H1.7. These results strongly suggest the importance of using a precise threshold based on ethnic-specific normal reference values for a correct classification of LV geometric patterns.
In the current study, the prevalence of LA dilatation tended to be lower, albeit not significantly, using thresholds from the healthy volunteer group than from guidelines when LAV was indexed to BSA, likely due to a higher threshold of LAV/BSA in the former than the latter in women (Table 3). However, LA dilatation was more common using thresholds from guidelines than from the healthy volunteer group when LAV was indexed to H2, again suggesting a possible overcorrection in the former. These results indicate that in addition to standard echocardiographic techniques, thresholds based on ethnic-specific normal reference values and a proper indexing algorithm are critical for a correct diagnosis of LVH and LA dilatation.
There were several limitations in this study. First, this was a cross-sectional study, and the effect of LV and LA remodelling patterns using different thresholds from the healthy volunteer group and guidelines on long-term outcomes of hypertensive patients needs to be explored using a prospective study design. Second, the sample size of hypertensive patients was not large enough and most patients received effective antihypertensive therapy, which may reduce the prevalence of LVH and abnormal LV and LA remodelling. Yet, the effect of different antihypertensive medications on LV and LA geometry was not determined. Further studies enrolling a large number of patients with different degrees of severity of hypertension are warranted.
In conclusion, using echocardiographic thresholds and indexing methods recommended by international guidelines may lead to significant misdiagnosis of LA dilatation, and LV abnormal geometry in Chinese patients with hypertension. As a correct diagnosis of LV and LA remodelling is vital for prognostic predictions and treatment decisions in hypertensive patients, thresholds based on ethnic-specific normal reference values and an accurate indexing algorithm are of paramount importance. Further studies addressing this question are warranted.
Supplementary data
Supplementary data are available at European Heart Journal - Cardiovascular Imaging online.
Funding
This work was supported by the National Research Program of China (2016YFC1300302), the Program of Introducing Talents of Discipline to Universities (BP 0719033), the State Key Program of National Natural Science of China (82030051), the International Collaboration and Exchange Program of China (81920108003), and the grants of the National Natural Science Foundation of China (81770442, 81970373, 82030051, 81770439, 81970377, 82000411, and 31770977).
Conflict of interest: There is no conflict of interest.
Data availability
The data underlying this article are available in the article and in its online supplementary material.
References
The Echocardiographic Normal Ranges Meta-Analysis of the Left heart (EchoNoRMAL) Collaboration.
Author notes
Yuanyuan Sheng, Mengmeng Li and Mingjun Xu contributed equally to this manuscript.

{kind=link}
{kind=link}
{kind=link}
{kind=link}