





This Spot the Diagnosis article refers to ‘Question: A mysterious cause of myocardial infarction: look beyond his coronary vessels’, by G.H.T. Kwok and K.K.H. Kam, https://doi.org/10.1093/ehjacc/zuae117.
Answer: B—polyarteritis nodosa
Explanation
Our patient’s angiogram exhibited features of ectatic looking coronary arteries in his left anterior descending artery (LAD), left circumflex artery (LCx), and proximal to mid segments of right coronary artery (RCA), with distal LCx showing an organized thrombus (Figure 1).
Beyond his ectatic coronary arteries, erythematous nodules in his hands raised suspicion of underlying vasculitis (Figure 2). Upon review of his past history, our patient satisfies 5 out 10 of the American College of Rheumatology (ACR) criteria for polyarteritis nodosa [1]. He has a history of rash suspicious of nodules or livedo reticularis, testicular tenderness, diastolic blood pressure > 90 mmHg, hepatitis B, and an arteriogram with aneurysm or occlusions of visceral arteries [2].
Treatment
For his coronary thrombosis with ectasia, anticoagulation with dabigatran was commenced, after discussing the risks of recurrent thrombosis vs. bleeding.
He was treated with six doses of 500 mg i.v. methylprednisolone, then started on prednisolone 60 mg daily, given 1000 mg i.v. cyclophosphamide for 5 cycles, and then maintained in remission with adalimumab and prednisolone 3 mg daily. Additionally, he was also prescribed entecavir for hepatitis B treatment, and cotrimoxale as prophylaxis for pneumocystis pneumonia.
Conclusion
Coronary artery involvement in polyarteritis nodosa is often overlooked. Previous literature has demonstrated cases of coronary ectasia, aneurysms, as in our case. Mainstay of management for coronary involvement would include anticoagulation and immunosuppressants for his underlying disease of polyarteritis nodosa (Figures 1–3).


Ectasia was found in all major coronary vessels on coronary angiography.

Upon preparing him for a right radial approach for coronary angiogram, the appearance of his hands was also noted. Circular macular rash on his hands were suggestive of an underlying inflammatory process against small blood vessels.
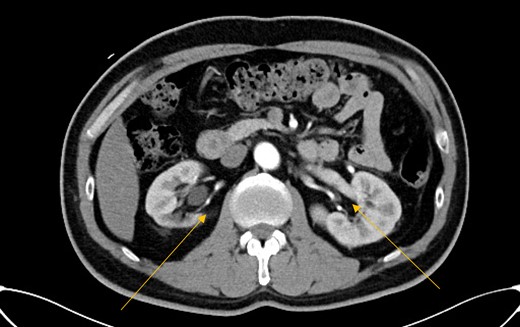
CT abdomen showing saccular aneurysms at renal arteries.
Funding
None declared.
Data availability
No new data were generated or analysed in support of this research.
References
Author notes
Conflict of interest: none declared

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comments