Abstract
Alterations in body composition are common among patients with Crohn’s disease (CD) and may represent a modifiable risk factor for dismal postoperative outcomes. This study aimed to investigate the association of preoperative body composition with postoperative complications and endoscopic postoperative recurrence (ePOR) in CD patients following ileocolic (re-)resection (ICR).
CD patients (≥16 years) scheduled for ICR with a preoperative CT or MRI scan (<12 months prior to ICR) were identified from an ongoing prospective, multicenter cohort study. Cross-sectional area normalized for body height (i.e. index) and lipid content (i.e. radiation attenuation on CT or signal intensity on MRI) of sketelal muscle (SM), subcutaneous adipose (SAT), and visceral adipose tissue (VAT) were analyzed at L3 level. Cut-offs were based on sex-specific tertiles. The primary outcome was postoperative complications (Clavien-Dindo grade I-IV) within 30 days. Secondary outcomes were moderate-to-severe complications (Clavien-Dindo grade ≥II), infectious complications (intra- or extra-abdominal), and ePOR (modified Rutgeerts’ score ≥i2b) at six months postoperatively. Multivariable logistic regression was performed to assess the association of preoperative body composition with study outcomes.
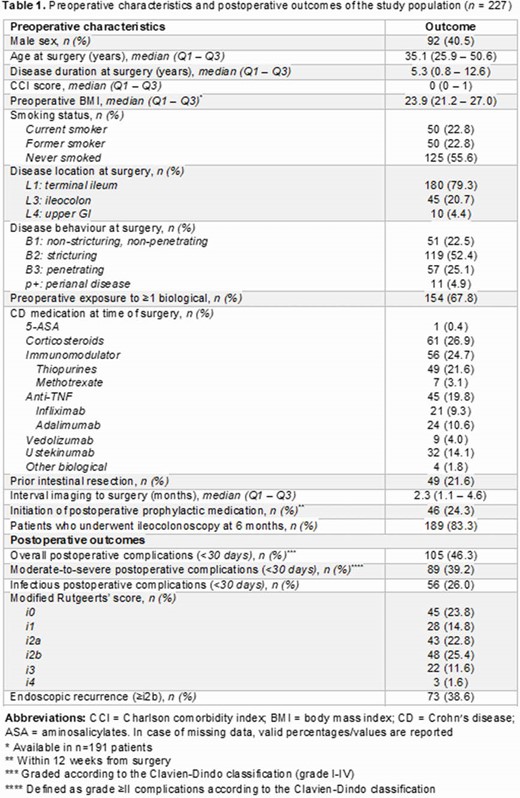
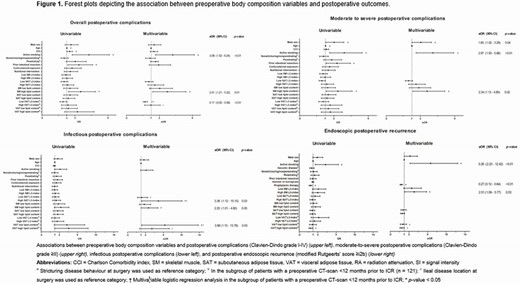
In total, 227 patients were included. Preoperative characteristiscs and postoperative outcomes are shown in Table 1. Median interval from preoperative imaging to ICR was 2.3 months (IQR 1.1–4.6). High lipid content of SM (i.e. myosteatosis) was associated with postoperative complications (aOR 2.51; 95%CI 1.21–5.22), moderate-to-severe complications (aOR 2.34; 95%CI 1.13–4.85), and infectious complications (aOR 2.20; 95%CI 1.01–4.80) (Figure 1). Low VAT-index was protective against postoperative complications (aOR 0.17; 95%CI 0.05–0.58). Low lipid content of VAT (aOR 3.98; 95%CI 1.15–13.78) and a high SAT-index (aOR 3.38; 95%CI 1.12–10.15) were associated with infectious complications. High SM-index was associated with ePOR (aOR 2.51; 95%CI 1.09–5.77). Preoperative body mass index (BMI) showed no association with study outcomes in uni- and multivariable analyses.
Preoperative myosteatosis on abdominal imaging is consistently associated with postoperative complications in patients with CD following ICR. Low VAT-index was identified as protective factor for postoperative complications, while low lipid content of VAT and a high SAT-index were associated with infectious complications. Surprisingly, high SM increased the risk of ePOR. Future research should identify strategies for preoperative improvement of body composition, rather than relying solely on BMI, and investigate if these improvements correlate with better postoperative outcomes.