Abstract
Up to 50% of patients with Crohn’s disease (CD) will require surgery, and 70-90% experience endoscopic recurrence within the first year postoperatively (1). Despite various treatments, there is scant data on the comparative efficacy to prevent recurrence (2). This study aims to compare the efficacy of medical treatments in preventing PORCD.
A comprehensive literature review was conducted using Medline, Embase, and the Cochrane Library through October 1, 2024. We included RCTs and prospective cohort studies, excluding pediatric studies, single-arm trials, and dose-comparison studies. The primary endpoint was assessing endoscopic recurrence (ER) (RS ≥i2), and secondary outcome was clinical recurrence (CDAI ≥150, Hanauer’s score ≥2, HBI ≥8) at 6, 12, and ≥18 months postoperatively. Frequentist random-effects network meta-analysis was conducted, reporting OR with 95% CI.
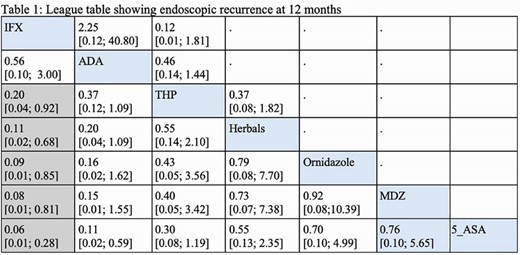
A total of 42 studies were included in this meta-analysis, 38 of which were RCTs, with 2,260 patients with CD. At 6 months, ADA showed the lowest ER (SUCRA= 84.5%), followed by VDZ (74.5%). ADA significantly reduced ER compared to thiopurine (OR = 0.33 [95% CI, 0.12–0.91]), probiotics (OR = 0.17 [95% CI, 0.03–0.99]), and vitamin D (OR = 0.07 [95% CI, 0.01–0.37]). VDZ did not significantly differ from thiopurine, ADA or MDZ. At 12 months, IFX (SURCA= 93%) and ADA (SUCRA= 90%) had the lowest ER, with IFX showing significant reductions compared to thiopurine, MDZ, 5-ASA, ornidazole, and herbals (table1). Similar findings were observed at 18 months, with IFX and ADA maintaining the lowest ER rates. For clinical recurrence, no significant differences were observed among therapies at 6 months. However, at 12 months, ADA and IFX were superior to most therapies, including thiopurine, MTX, and budesonide. By 18 months, ADA had significantly less clinical recurrence than IFX (OR = 0.06 [95% CI, 0.01–0.50]).
Anti-TNFs are more effective than other therapies in preventing post-op CD recurrence. VDZ did not outperform thiopurines. Further RCTs are needed to evaluate newer therapies for post-op CD management.
1.Spinelli A, Sacchi M, Fiorino G, Danese S, Montorsi M. Risk of postoperative recurrence and postoperative management of Crohn’s disease. World J Gastroenterol. 2011;17(27):3213-3219. doi:10.3748/wjg.v17.i27.3213
2.Fasulo E, D’Amico F, Osorio L, et al. The Management of Postoperative Recurrence in Crohn’s Disease. J Clin Med. 2023;13(1):119. Published 2023 Dec 25. doi:10.3390/jcm13010119