




Abstract
Patients with inflammatory bowel disease (IBD) bear an increased colorectal cancer (CRC) risk. This risk is further increased following colonic low-grade dysplasia (LGD). Endoscopic surveillance programs aim to reduce CRC risk by detecting and removing precancerous lesions like LGD. Long-term risk of high-grade dysplasia (HGD) or CRC after LGD is relatively unknown, since most available studies are small and cover a relatively short follow-up period. We established a nationwide cohort of IBD patients with LGD to determine long-term cumulative advanced neoplasia (HGD and/or CRC) incidence, and to identify risk factors for advanced neoplasia development.
All IBD patients with LGD between 1991 and 2005 in the Netherlands were identified using the Dutch National Pathology Registry (PALGA). Follow-up data were collected until January 2016. The cumulative incidence of advanced neoplasia was determined by Kaplan–Meier curves, censoring patients at the end of colorectal surveillance or (sub)total colectomy. Risk factors for developing advanced neoplasia were identified with multivariable Cox regression analysis.
We identified 2738 patients with colonic LGD with a median follow-up of 9.5 years (IQR 4.2–13.7 years) after initial LGD diagnosis (1981 (72.4%) ulcerative colitis, 541 (19.8%) Crohn’s disease, 215 (7.9%) indeterminate colitis). 423 (15.5%) patients underwent (sub)total colectomy. Advanced neoplasia was detected in 397 of 2738 patients, including 240 patients with CRC. The cumulative incidence of advanced neoplasia was 3.5%, 9.1%, 14.4%, 21.9%, and 29.9% after 1, 5, 10, 15, and 20 years, respectively (Figure 1). Median time to develop advanced neoplasia after LGD was 4.7 years (IQR 1.3–10.0 years). Multivariable analysis identified a higher age (> 55 years) at initial LGD (hazard ratio (HR) 1.87; 95% confidence interval (CI) 1.53–2.30), an IBD duration > 5 years before LGD (HR 1.46; 95% CI 1.13–1.90) and male gender (HR 1.37; 95% CI 1.10–1.71) as independent risk factors for advanced neoplasia following LGD.
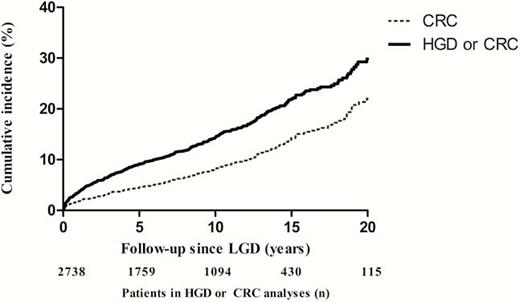
Cumulative incidence of high-grade dysplasia and/or colorectal cancer following low-grade dysplasia in patients with inflammatory bowel disease.
In a large nationwide cohort of IBD patients with LGD with median follow-up of almost 10 years, the cumulative incidence of advanced neoplasia was 21.9% after 15 years. Older age at LGD (> 55 years), longer IBD duration (>5 years) before LGD, and male gender were independent risk factors for advanced neoplasia development after initial LGD. These results may aid in risk stratification for endoscopic surveillance after LGD in patients with IBD.



{kind=link}