Abstract
Double aortic arch (DAA) is a relatively rare vascular malformation that causes few problems in adults. However, the presence of DAA makes esophageal cancer surgery difficult, especially during upper mediastinal dissection. Here we report a bilateral thoracoscopic surgical technique in a patient with highly advanced esophageal cancer complicated with DAA.
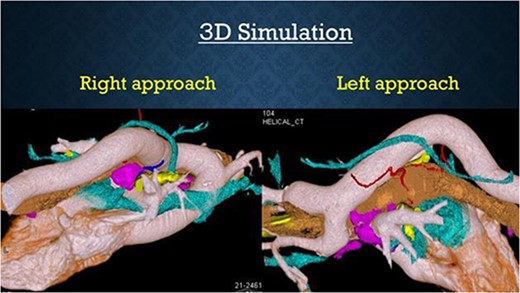
73-year-old male, cT3N4M0 stage III (UICC-TNM 7th) mid-thoracic esophageal cancer with DAA was diagnosed. After two courses of neoadjuvant chemotherapy, surgical treatment was planned. To develop a surgical strategy for esophagectomy for this complex malformation, we created a 3D printer model of the case. The results suggested that a bilateral thoracoscopic approach in the prone position was the ideal approach for upper mediastinal dissection. As expected, it was difficult to dissect the upper mediastinum using only a right-sided approach, especially on the esophagus oral side behind the right aortic arch (RAA), where dissection from the right side was impossible. By adding a left lateral approach, the oral side of the esophagus was pulled in from the left aortic arch (LAA) and was easily dissected. The operation was successful and the postoperative course was uneventful. In this presentation, we will demonstrate the technique of bilateral approach for advanced esophageal cancer complicated with DAA.
The surgical strategy for patients with thoracic esophageal cancer and a coexisting complex vascular anomaly known as a double aortic arch (DAA) is a highlight. Typically, surgical approaches have been limited to either left or right thoracic access. However, through preoperative simulation using 3D printing, a bilateral approach was deemed safe and effective for these cases. The 3D printer models provided invaluable insights into the anatomical relationships of blood vessels, trachea, and heart, allowing for precise planning and execution of the surgery. Challenges such as the proximity of the descending aorta to the trachea and the optimal approach angle were successfully addressed through simulation, enhancing surgical outcomes. Furthermore, the bilateral thoracoscopic approach demonstrated potential benefits in preserving delicate structures like the recurrent laryngeal nerve. This innovative use of 3D printing technology in preoperative planning represents a significant advancement in the field of gastrointestinal surgery, offering improved safety and precision for patients with complex anatomical variations like DAA.
3D printer is useful for simulating thoracoscopic esophagectomy with macrovascular malformations. Bilateral approach is appropriate for surgery of esophageal cancer complicated with DAA and a 3D printer is a useful tool for simulating esophageal surgery.