






Abstract
The spectrum of infections caused by methanogens remains to be described. We searched for methanogens in the blood of febrile patients using specific tools.
Blood culture samples routinely collected in patients with fever were prospectively screened by specific PCR assays for methanogens. Positive samples were observed by autofluorescence and electron microscopy, analyzed by metagenomics and cultured using previously developed methods. Blood culture bottles experimentally inoculated were used as controls. The presence of methanogens in vascular and cardiac tissues was assessed by indirect immunofluorescence, fluorescent in situ hybridization and PCR-based investigations.
PCR detection attempted in 7,716 blood samples, was negative in all 1,312 aerobic bottles and 810 bacterial culture-negative anaerobic bottles. PCRs were positive in 27/5,594 (0.5%) bacterial culture-positive anaerobic bottles collected from 26 patients. Sequencing confirmed Methanobrevibacter smithii associated with staphylococci in 14 patients, Enterobacteriaceae in nine patients and streptococci in three patients. Metagenomics confirmed M. smithii in five samples, and M. smithii was isolated in broth from two samples; the genomes of these two isolates were sequenced. Blood cultures experimentally inoculated with Enterobacteriaceae, Staphylococcus epidermidis or Staphylococcus hominis yielded hydrogen, but no methane, authentifying observational data. Three patients diagnosed with infectious mitral endocarditis, were indisputably diagnosed by microscopy, PCR-based detections and culture: we showed M. smithii microscopically and by a specific PCR followed by sequencing method in two of three cardiovascular tissues.
Using appropriate laboratory methods, M. smithii is demonstrated as causing archaemia and endocarditis in febrile patients who are coinfected by bacteria.
Archaea are prokaryotes that are distinct from bacteria and eukaryotes and have been studied mainly in environmental microbiology [1]. However, in humans, archaeal methanogens (here, referred to as methanogens) play an important physiological role, especially in the digestive tract, by producing methane from the hydrogen emitted by anaerobic bacteria [2]. Methanogens are difficult to detect because the primers used for detection and identification of bacteria based on 16S ribosomal DNA (rDNA) are not efficient for methanogens. Additionally, the DNA extraction process for methanogens is different from the process that is routinely used for bacteria. This led us to describe specific tools for the detection of methanogens [3]. Moreover, methanogens and members of the genus Methanobrevibacter need hydrogen, are extremely oxygen-sensitive, and require an anaerobic atmosphere for culture. Over the last 10 years, only 5 teams have reported the culture of methanogens from human samples [4–8]. We previously developed a simplified culture technique that allows aerobic growth that does not require specific equipment [9].
Due to these challenges in the detection of methanogens in pathological situations, their clinical spectrum is unknown. The first studies to report their presence in cerebral abscesses [10, 11], muscle abscesses [12], and vaginosis [13] were quite recent and have only been reported by our team. Moreover, until very recently, methanogens have been isolated via culture and polymerase chain reaction (PCR) analysis in urine [14] and milk [15].
We aimed to evaluate the presence of methanogens in the blood of febrile patients. Here, we demonstrate the presence of methanogens in the blood of 26 febrile patients, including 3 patients who were diagnosed with infective endocarditis.
METHODS
Blood Culture Collection
This prospective study used blood culture samples that were collected at the diagnostic laboratory of Institut Hospitalier Universitaire Mediterranée Infection as a part of routine activities (September 2018–April 2020) and was approved by the Institut Hospitalier Universitaire Méditerranée Infection Ethics Committee. We specifically tested the anaerobic bottles (BacT/ALERT FN Plus, bioMérieux, Lyon, France) incubated into the BACT/ALERT VIRTUO apparatus (bioMérieux) and hypothesized that methanogens that would have otherwise gone unnoticed could be found with anaerobic hydrogen-producing bacteria (Figure 1). We also tested the blood cultures in aerobic bottles (BacT/ALERT FA Plus, bioMérieux) and in anaerobic bottles that were negative for bacteria as negative controls. To roughly evaluate the incidence of methanogen archaemia, we tested all aerobic and anaerobic blood culture bottles that were positive or negative for 1 week. The purpose of this evaluation was to model the 150 000 blood culture bottles that we receive annually, as our laboratory serves an area with 500 000 inhabitants. Finally, we evaluated the prevalence of methanogens in the blood of febrile patients diagnosed with infective endocarditis vs other febrile patients using our specific kit [16].
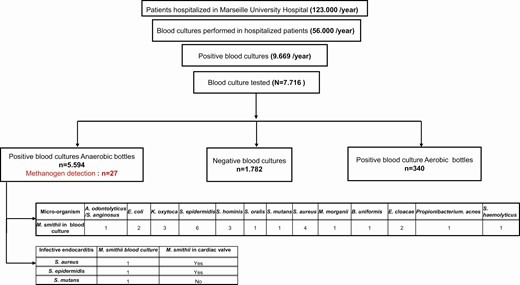
Study workflow and the main results. *Methanogen detection indicated in red.
Detection of Methanogens in Blood Cultures
Total DNA extracted from blood culture samples and from negative controls was evaluated with PCR sequencing of the archaeal 16S ribosomal RNA (rRNA) as previously described [3]. All anaerobic blood cultures that were positive for bacteria were tested after 10-day storage at room temperature, including a subset of 1671 anaerobic blood cultures also tested immediately after positive detection of bacteria using the BACT/ALERT VIRTUO apparatus. Real-time PCR assays that specifically target the Methanobrevibacter smithii rpoB and 16S rRNA genes were performed as confirmatory tests as previously described [3]. Autofluorescent methanogens were microscopically observed in PCR-positive blood culture as previously described [17]. As for electron microscopy observations, 100 µL of PCR-positive blood culture sample was fixed with 2.5% glutaraldehyde, spotted onto a glass slide by cytocentrifugation (Shandon Cytospin 4, Thermo Scientific, Waltham, MA), stained using 1% phosphotungstic acid (Sigma Aldrich, Saint-Louis, MO) for 2 minutes at room temperature, and observed using a TM4000Plus scanning electron microscope (Hitachi, Tokyo, Japan). We performed metagenomics to evaluate the complete repertoire of microorganisms in 12 methanogen PCR-positive blood cultures and 1 negative control. Samples were lysed in the presence of acid-washed powder glass beads (G4649-500g, Sigma Aldrich) and disruption medium (Scientific Industries In., Bohemia, NY) using a FastPrep-24 5G Grinder (mpBio, Illkirch-Graffenstaden, France) at 6.5 m/s for 90 s. Then, DNA was extracted following 1 of 3 protocols: protocol 1 included protease incubation and purification using the EZNA tissue DNA kit (Omega Biotek Inc, Norcross, GA); protocol 3 was as previously described [18]; and protocol 5 included deglycosylation and purification using the EZ1 Advanced XL device (Qiagen, Courtaboeuf, France) as previously described [19]. DNA extracted using protocols 1 or 5 was PCR-amplified for the V3-V4 region of the bacterial 16S rRNA gene, and DNA extracted using protocol 3 was amplified for the V3-V4 region of the archaeal 16S rRNA gene. Amplified DNAs were pooled, bar coded, and sequenced with MiSeq technology with a paired-end strategy (Illumina Inc, San Diego, CA). Reads were blasted against the 16S microbial database, with a coverage 99% threshold for bacterial V3-V4 and 95% threshold for archaeal 16S rDNA [20].
Experimentally Inoculated Blood Cultures
We tested the production of hydrogen and methane by the bacteria isolated via culture from M. smithii PCR-positive anaerobic blood cultures. Precautional degassed anaerobic bottles were inoculated with sterile blood from healthy donors (tested negative for methanogens by PCR), coinoculated with 106M. smithii or with 106 bacteria coisolated with M. smithii, or coinoculated with bacteria and M. smithii. Bottles incubated under the same conditions as for clinical samples were monitored using M. smithii real-time PCR and by measuring hydrogen and methane production at day 1, 3, 5, 7, and 10. Gas was measured in 0.1 cm3 sampled from the bottles using a gastight syringe, injected into a shincarbon ST 80/100 micropacked column. Hydrogen was detected in the negative polarity using argon as the reference gas; methane was detected in the positive polarity using helium as the reference gas in a Clarus 580 gas chromatograph (Perkin Elmer, Villebon-sur-Yvette, France). Data recording and processing were performed using TotalChrom 6.3.2 software (Perkin Elmer). Experiments were performed in triplicate. In order to test the susceptibility of M. smithii to oxygen, 105M. smithii archaea were inoculated into 1 mL phosphate buffered saline (PBS) and 1 mL of Ae/Ana transport medium. One tube of each series (with PBS or Ae/Ana medium) was subcultured in a Hungate tube (Dominique Dutscher, Brumath, France) that contained 5 mL of SAB medium supplemented with 20% carbon dioxide and 80% hydrogen after a 5-minute exposure to oxygen [21]. Additional tubes were subcultured under the same conditions after 10 minutes, 15 minutes, 20 minutes, and 30 minutes exposure to oxygen. Growth of M. smithii was assessed by measuring methane production after a 3-day incubation at 37°C.
Isolation, Identification, and Characterization of Blood Isolates
Methanogens were cultured from blood culture samples in an aerobic atmosphere as previously described [9]. Methanogen colonies observed after an 8-day incubation at 37°C were isolated for DNA extraction and sequenced using MiSeq (Illumina Inc). Genome sequence assembly was performed using GapCloser [22], Spades [23], and Trimmomatic [24] software packages and annotated using Prokka [25] to produce an M. smithii Roary pangenome that incorporated a global dataset of 29 M. smithii genomes that were downloaded from the National Center for Biotechnology Information [26]. Draft genome sequences of the M. smithii strain BC84 and strain BC55 have been deposited in the European Nucleotide Archive under accession numbers CAACAE010000001 and CAAKMW010000001, respectively.
Cardiac Valve and Aortic Tissue Pathology
Indirect immunofluorescence was performed using M. smithii-immunized rabbit serum and a goat anti-rabbit immunoglobulin G antibody conjugated with fluorescein (ImmuniReagents Inc, Raleigh, NC), which included a degenerative fibrous and calcified aortic valve as a negative control. We also performed fluorescent in situ hybridization on cardiac valve and aortic tissues using the green fluorescent probe Arc915 targeting all methanogens and the red fluorescent bacteria-specific probe EUB338 as previously described [27]. Further, total DNA was extracted from 2 cardiac valves (patients 3 and 7) and 1 surgical aortic sample (patient 11) using method 1, as above. As this protocol failed to detect methanogen DNA in the surgical aortic sample, an additional method of DNA extraction was performed to eliminate the presence of eventual inhibitors of nucleic acid amplification. In the presence of an aortic sample from a patient with M. smithii-negative blood cultures as a negative control, we incubated a small piece of aortic sample from patient 11 with proteinase K and lysis buffer for 2 hours at 56°C. The lysate mixture was migrated on a 1.5% agarose gel electrophoresis containing SYBR Safe (Thermo Fisher, Illkirch-Graffenstaden, France), and DNA fragments were cut from the gel. Purification and extraction of total DNA were carried out using the QIAquick Gel Extraction Kit (Qiagen; method 2). PCR followed by sequencing was performed to tentatively amplify the archaeal 16S rRNA as previously described [3]. Further, a homemade quantitative real-time PCR system to target a 153-bp fragment of the methanogen 16S rRNA gene was designed and validated in order to improve the sensitivity of methanogen DNA detection (Supplementary Table 1). Human β-actin internal DNA extraction control PCR detection was performed for each sample.
Statistical Analyses
We compared age, sex, department, microorganism, and mortality among 3 patients with endocarditis with M. smithii-positive PCR results of blood and 3 control patients with endocarditis M. smithii-negative PCR results. Controls were time-matched to cases as closely as possible. Data collected from the patient charts were recorded in an Excel document. The analyses were performed using R Software (version 3.2.3). Categorical variables were compared using the Fisher t test. Differences were considered significant when P < .05.
RESULTS
Detecting M. smithii in Blood Cultures
Among 7716 tested blood cultures, all 1312 aerobic cultures tested negative for methanogen by PCR, 27/5424 (0.5%) anaerobic cultures positive for bacteria tested positive for methanogen by PCR, and no methanogens were detected in more than 810 anaerobic bottles that were negative for bacteria. Noteworthy, the 27 methanogen PCR-positive blood cultures tested positive after 10-day storage at room temperature, whereas 1671 such blood culture bottles remained PCR-negative when tested immediately after BACT/ALERT VIRTUO positive detection. In all of the 27 methanogen PCR-positive blood cultures, 16S rRNA gene amplicon sequencing identified M. smithii, and M. smithii–specific real-time PCR analyses confirmed these results. Further, metagenomic studies detected M. smithii in 3 bottles by using 2 detection systems, and 2 additional bottles were slightly positive, as confirmed by a single detection system (Supplementary Table 2). The percentage of M. smithii reached approximately 13% of the total reads in a blood culture collected from patient 2. Interestingly, 2 blood cultures collected from patient 4 were both positive. Autofluorescent forms with shapes and sizes like those of M. smithii were observed in PCR-positive blood cultures but not in PCR-negative blood cultures (Figure 2). Scanning electron microscopy showed 2 forms in each PCR-positive blood culture; 1 form corresponded to the bacteria cocultured with M. smithii, and the second form was characterized by a microbial cell diameter <700 µm and an irregular contour, which is characteristic of M. smithii (Figure 2). Indeed, the 27 PCR-positive blood cultures grew Staphylococcus epidermidis (n = 6), Staphylococcus aureus (n = 4), Staphylococcus hominis (n = 3), Staphylococcus haemolyticus (n = 1), Streptococcus oralis (n = 1), Streptococcus mutans (n = 1), Escherichia coli (n = 2), Enterobacter cloacae (n = 2), Bacteroides uniformis (n = 1), Propionibacterium acnes (n = 1), Klebsiella oxytoca (n = 3), Morganella morganii (n = 1), Actinomyces odontolyticus (n = 1), and Streptococcus sanguinis (n = 1). We then tested 922 negative blood cultures (400 aerobic and 522 anaerobic) and 260 positive blood cultures, which included 90 aerobic culture-positive and 170 anaerobic culture-positive bottles, in 1 week. Anaerobic culture-negative bottles and aerobic culture-negative and culture-positive bottles were PCR-negative for the methanogen 16S rRNA gene; however, 1/170 (0.6%) anaerobic culture-positive bottles was PCR-positive for the methanogen 16S rRNA gene.
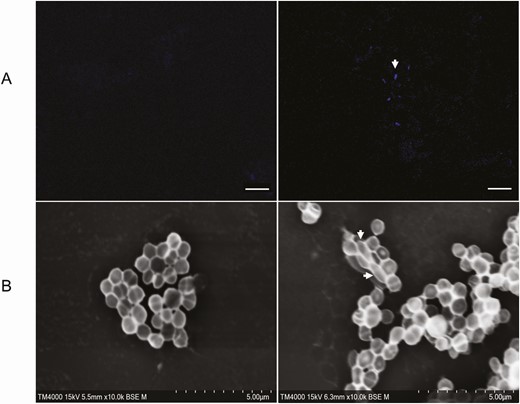
Microscopic detection of Methanobrevibacter smithii in 1 patient with mixed Staphylococcus aureus and M. smithii infective endocarditis (patient 11). A, Autofluorescent M. smithii methanogens in the blood were excited by an ultraviolet excitation laser, and image acquisition was performed with a Zeiss LSM 800 confocal microscope using a 63 X, 1.4 numeric aperture oil immersion objective. The scale bar represents 10 µm. B, Methanobrevibacter smithii methanogens in the blood were observed along with S. aureus using scanning electron microscopy with TM4000Plus software (Hitachi). All image settings for the magnification, focus, and keV mode are shown on micrographs. Scale bars represent 5 μm. Left panels, negative controls; right panels, patient’s blood sample.
Hydrogen Production by Bacteria Codetected With M. smithii
Anaerobic bottles experimentally inoculated with sterile blood remained negative for methane and M. smithii PCR detection, as well as anaerobic bottles inoculated with sterile blood and bacteria. As for hydrogen, we detected traces of hydrogen in noninoculated anaerobic bottles, whereas bottles inoculated with M. morganii, E. coli, S. hominis, S. epidermidis, K. oxytoca, and Enterobacter cloacae produced significantly more hydrogen than these controls (Supplementary Figure 1). Finally, M. smithii that was exposed for 15–30 minutes to oxygen did not grow further in PBS or Ae/Ana medium (Supplementary Figure 2).
Patients
The 27 M. smithii–positive blood cultures were collected in 26 patients, as 2 M. smithii–positive blood cultures were collected in patient 4 (Table 1). Six patients had septic shock, 5 digestive tract injury, 2 postchemotherapy fever, 2 pneumonia, and 2 influenza. Healthcare-associated infection diagnosed in 6 patients included 2 operative site infections, 2 vascular catheter infections, and 2 urinary tract infections. Fifteen patients had received antibiotics and 4 had received blood transfusion before M. smithii–positive blood culture. Four died during hospitalization. In this series, 3 patients remarkable for having infectious mitral endocarditis are detailed (Supplementary Appendix), corresponding to an incidence of archaemia of 10% among the 30 infectious endocarditis patients tested.
Characteristics of 26 Patients Diagnosed With Methanobrevibacter smithii Archaemia
| Case | Age, y | Sex | Bacterial Culture | Methanobrevibacter smithii culture | Medical History | Risk Factor | Digestive Symptoms | Central Catheter | Previous Antibiotics | Previous Antibiotic Regimen | Second-line Antibiotics | Appropriate Antibiotica | Survived |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 60 | F | Staphylococcus hominis | Negative | Influenza B during a return to Mecca | None | Yes | No | No | Amoxicillin + clavulanic acid | No | Yes | |
| 2 | 45 | M | Streptococcus oralis | Negative | Central venous catheter infection | Lingual carcinoma chemotherapy and immunotherapy | No | Yes | No | Imipenem + linezolid | No | No; 4 months | |
| 3 | 44 | F | Streptococcus mutans | Positive | Infectious endocarditis on the native mitral valve | None | No | No | Yes | Vancomycin + gentamicin | Ceftriaxone + gentamycin | No | Yes |
| 4 | 60 | F | Klebsiella oxytoca | Negative | Septic shock and occlusive syndrome | Ovarian cancer in 2008 | Yes | Yes | Yes | Ceftriaxone metronidazole | Unchanged | Yes | Yes |
| 5 | 60 | M | S. hominis | Negative | Acute respiratory distress due to Streptococcus pneumoniae; left basal pneumonia | Chronic obstructive pulmonary disease | No | No | Yes | Cefotaxime | Unchanged | No | Yes |
| 6 | 78 | F | Escherichia coli | Negative | Obstructive pyelonephritis and septic shock | Bilateral breast cancer and metastatic colon cancer | No | Yes | Yes | Ticarcillin tazobactam | Imipenem | No | No. 1 day |
| 7 | 60 | M | Staphylococcus epidermidis | Positive | Infectious endocarditis on a mitral mechanical valve | Mitral mechanical; 1982 | Yes | No | Yes | Ofloxacin | Vancomycin + gentamycin | No | Yes |
| 8 | 57 | F | K. oxytoca | Negative | Progression of liver metastasis with febrile illness and abdominal pain | Carcinoid tumor of the small bowel with liver, pancreatic, bone, and mammary and lymph node metastases | No | Yes | No | Ticarcillin tazobactam | No | No. 2 days | |
| 9 | 55 | M | S. epidermidis | Negative | Epistaxis with thrombocytopenia, anemia, and fever on day 7 of chemotherapy and blood transfusion | Recurrence of Hodgkin’s lymphoma and chemotherapy | No | Yes | No | Ticarcillin tazobactam | No | Yes | |
| 10 | 59 | M | Actinomyces odontolyticus, Streptococcus anginosus | Negative | Septic shock secondary to hepatic abscess | Duodenal tumor treated by duodenopancreatectomy with choledocojejunal anastomosis in 2009 | Yes | No | No | Imipenem + gentamycin + vancomycin | No | Yes | |
| 11 | 80 | F | Staphylococcus aureus | Negative | Mitral native valve infective endocarditis complicated with aortic mycotic aneurysm of the renal aorta ruptured | Bilateral hip prosthesis, obesity, dysthyroidism | Yes | No | No | Oxacillin | No | No. 7 days | |
| 12 | 57 | M | Morganella morganii | Negative | Vascular surgery with iliofemoropopliteal bypass graft and cutaneous excision of skin lesion complicated with hemorrhage with blood transfusion | Right scarpa melanoma with vascular invasion | No | Yes | No | Cotrimoxazole | No | Yes | |
| 13 | 75 | F | S. hominis | Negative | Acute myeloblastic leukemia; fever after 24 hours of chemotherapy | Ovarian carcinoma in 2003 | No | Yes | Yes | Cotrimoxazole | Ticarcillin tazobactam | No | Yes |
| 14 | 72 | M | Enterobacter cloacae | Negative | Febrile occlusive syndrome due to the perforation of the posterior gastric wall involving a collection in the back cavity of the epiploons and a zone of renal parenchymal necrosis complicated with hemorrhage with blood transfusion | Attempted suicide by firearm, resulting in transfixing the gastric wound, hepatic wound, and retroperitoneal hematoma with hemorrhage | Yes | Yes | No | Ticarcillin tazobactam | No | Yes | |
| 15 | 71 | M | S. aureus | Negative | Nosocomial infection 3 weeks after neurosurgery for spinal arthrodesis for spondylodiscitis | Demyelinating Charcot-Marie-Tooth neuropathy | No | No | Yes | Vancomycin | Cotrimoxazole + clindamycin + Ofloxacin + rifampicin | Yes | Yes |
| 16 | 31 | M | S. epidermidis | Negative | High-speed road accident complicated by severe cranial tremor and the rupture of the aortic isthmus; fever and pneumonia 4 days after surgery | No | Yes | Yes | Amoxicillin + clavulanic acid | Cefepime | No | Yes | |
| 17 | 50 | F | Staphylococcus haemolyticus | Negative | Occlusive syndrome on peritoneal carcinoma surgery with lateral ileo-colic anastomosis central catheter ablation | Squamous cell carcinoma of the cervix with peritoneal metastases | Yes | Yes | No | Linezolid | No | Yes | |
| 18 | 2 | M | E. cloacae | Negative | Fever and septic shock | Liver transplant 8 months before for biliary atresia | No | Ye s | Yes | Ticarcillin tazobactam + Amikacin | Ticarcillin tazobactam + Amikacin | No | Yes |
| 19 | 50 | M | E. coli | Negative | Graft pyelonephritis urine culture E. coli | Kidney transplant for polycystic kidney disease 15 years earlier | No | No | Yes | Ceftriaxone + Ciprofloxacin | Ciprofloxacin | No | Yes |
| 20 | 38 | M | Bacteroides uniformis | Negative | Cephalic duodeno-pancreatectomy in the context of a neuroendocrine tumor complicated by hypovolemic shock, fever, splenic vein thrombosis, and small intestine necrosis; abdominal drainage culture: Enterococcus faecium, E. coli | Neuroendocrine tumor chemotherapy; biliary prosthesis 5 months before | Yes | Yes | Yes | Cefepime + Tigecycline | Ticarcillin tazobactam | No | Yes |
| 21 | 88 | M | Propionibacterium acnes | Negative | E. coli prostatitis and coma on epilepsy in the context of the antiepilepticus treatment interruption | Epilepsy benign prostatic hyperplasia | No | Yes | Yes | Amoxicillin + clavulanic acid | Ceftriaxone | No | Yes |
| 22 | 69 | M | S. aureus | Negative | Septic shock on the central catheter | Implantable defibrillator gastrostomy for swallowing disorder, multiple sclerosis | No s | Yes | Yes | Ceftriaxone + levofloxacin | Ticarcillin tazobactam + vancomycin | No | Yes |
| 23 | 49 | M | S. epidermidis | Negative | Septic shock complicated by renal failure and related to bacteremia with the implantable chamber | Bricker’s surgery at birth for congenital bladder atrophy, kidney transplant at age 37 years 2 years ago: colostomy for occlusive syndrome 1 month ago, complicated with removal of Bricker and nephrostomy | Yes | Yes | Yes | Cefepime + tigecycline | Tigecycline | No | Yes |
| 24 | 85 | F | S. aureus | Negative | S. aureus bacteremia on a venous catheter | Pulmonary arterial hypertension | No | Yes | Yes | Amoxicillin + Ticarcillin + tazobactam + Ceftriaxone | Ciprofloxacin | No | Yes |
| 25 | 81 | M | S. epidermidis | Negative | Influenza A and S. epidermidis bacteremia | Stage 4 right adrenal neuroblastoma with hepatic and bone involvement | No | Yes | Yes | Ceftriaxone | Vancomycin + Teicoplanin | No | Yes |
| 26 | 83 | F | S. epidermidis | Negative | Iron deficiency anemia with abdominal pain, fever 38°C, and vomiting; blood transfusion; fibroscopy: antral and fundic gastritis due to Helicobacter pylori, S. epidermidis bacteremia; ¼ blood culture | Pituitary macroadenoma complicated by insipidus diabetes osteosynthesis by centro medullary nail of the left femur 4 month ago | Yes | Yes | No | Ceftriaxone | Unchanged | No | Yes |
| Case | Age, y | Sex | Bacterial Culture | Methanobrevibacter smithii culture | Medical History | Risk Factor | Digestive Symptoms | Central Catheter | Previous Antibiotics | Previous Antibiotic Regimen | Second-line Antibiotics | Appropriate Antibiotica | Survived |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 60 | F | Staphylococcus hominis | Negative | Influenza B during a return to Mecca | None | Yes | No | No | Amoxicillin + clavulanic acid | No | Yes | |
| 2 | 45 | M | Streptococcus oralis | Negative | Central venous catheter infection | Lingual carcinoma chemotherapy and immunotherapy | No | Yes | No | Imipenem + linezolid | No | No; 4 months | |
| 3 | 44 | F | Streptococcus mutans | Positive | Infectious endocarditis on the native mitral valve | None | No | No | Yes | Vancomycin + gentamicin | Ceftriaxone + gentamycin | No | Yes |
| 4 | 60 | F | Klebsiella oxytoca | Negative | Septic shock and occlusive syndrome | Ovarian cancer in 2008 | Yes | Yes | Yes | Ceftriaxone metronidazole | Unchanged | Yes | Yes |
| 5 | 60 | M | S. hominis | Negative | Acute respiratory distress due to Streptococcus pneumoniae; left basal pneumonia | Chronic obstructive pulmonary disease | No | No | Yes | Cefotaxime | Unchanged | No | Yes |
| 6 | 78 | F | Escherichia coli | Negative | Obstructive pyelonephritis and septic shock | Bilateral breast cancer and metastatic colon cancer | No | Yes | Yes | Ticarcillin tazobactam | Imipenem | No | No. 1 day |
| 7 | 60 | M | Staphylococcus epidermidis | Positive | Infectious endocarditis on a mitral mechanical valve | Mitral mechanical; 1982 | Yes | No | Yes | Ofloxacin | Vancomycin + gentamycin | No | Yes |
| 8 | 57 | F | K. oxytoca | Negative | Progression of liver metastasis with febrile illness and abdominal pain | Carcinoid tumor of the small bowel with liver, pancreatic, bone, and mammary and lymph node metastases | No | Yes | No | Ticarcillin tazobactam | No | No. 2 days | |
| 9 | 55 | M | S. epidermidis | Negative | Epistaxis with thrombocytopenia, anemia, and fever on day 7 of chemotherapy and blood transfusion | Recurrence of Hodgkin’s lymphoma and chemotherapy | No | Yes | No | Ticarcillin tazobactam | No | Yes | |
| 10 | 59 | M | Actinomyces odontolyticus, Streptococcus anginosus | Negative | Septic shock secondary to hepatic abscess | Duodenal tumor treated by duodenopancreatectomy with choledocojejunal anastomosis in 2009 | Yes | No | No | Imipenem + gentamycin + vancomycin | No | Yes | |
| 11 | 80 | F | Staphylococcus aureus | Negative | Mitral native valve infective endocarditis complicated with aortic mycotic aneurysm of the renal aorta ruptured | Bilateral hip prosthesis, obesity, dysthyroidism | Yes | No | No | Oxacillin | No | No. 7 days | |
| 12 | 57 | M | Morganella morganii | Negative | Vascular surgery with iliofemoropopliteal bypass graft and cutaneous excision of skin lesion complicated with hemorrhage with blood transfusion | Right scarpa melanoma with vascular invasion | No | Yes | No | Cotrimoxazole | No | Yes | |
| 13 | 75 | F | S. hominis | Negative | Acute myeloblastic leukemia; fever after 24 hours of chemotherapy | Ovarian carcinoma in 2003 | No | Yes | Yes | Cotrimoxazole | Ticarcillin tazobactam | No | Yes |
| 14 | 72 | M | Enterobacter cloacae | Negative | Febrile occlusive syndrome due to the perforation of the posterior gastric wall involving a collection in the back cavity of the epiploons and a zone of renal parenchymal necrosis complicated with hemorrhage with blood transfusion | Attempted suicide by firearm, resulting in transfixing the gastric wound, hepatic wound, and retroperitoneal hematoma with hemorrhage | Yes | Yes | No | Ticarcillin tazobactam | No | Yes | |
| 15 | 71 | M | S. aureus | Negative | Nosocomial infection 3 weeks after neurosurgery for spinal arthrodesis for spondylodiscitis | Demyelinating Charcot-Marie-Tooth neuropathy | No | No | Yes | Vancomycin | Cotrimoxazole + clindamycin + Ofloxacin + rifampicin | Yes | Yes |
| 16 | 31 | M | S. epidermidis | Negative | High-speed road accident complicated by severe cranial tremor and the rupture of the aortic isthmus; fever and pneumonia 4 days after surgery | No | Yes | Yes | Amoxicillin + clavulanic acid | Cefepime | No | Yes | |
| 17 | 50 | F | Staphylococcus haemolyticus | Negative | Occlusive syndrome on peritoneal carcinoma surgery with lateral ileo-colic anastomosis central catheter ablation | Squamous cell carcinoma of the cervix with peritoneal metastases | Yes | Yes | No | Linezolid | No | Yes | |
| 18 | 2 | M | E. cloacae | Negative | Fever and septic shock | Liver transplant 8 months before for biliary atresia | No | Ye s | Yes | Ticarcillin tazobactam + Amikacin | Ticarcillin tazobactam + Amikacin | No | Yes |
| 19 | 50 | M | E. coli | Negative | Graft pyelonephritis urine culture E. coli | Kidney transplant for polycystic kidney disease 15 years earlier | No | No | Yes | Ceftriaxone + Ciprofloxacin | Ciprofloxacin | No | Yes |
| 20 | 38 | M | Bacteroides uniformis | Negative | Cephalic duodeno-pancreatectomy in the context of a neuroendocrine tumor complicated by hypovolemic shock, fever, splenic vein thrombosis, and small intestine necrosis; abdominal drainage culture: Enterococcus faecium, E. coli | Neuroendocrine tumor chemotherapy; biliary prosthesis 5 months before | Yes | Yes | Yes | Cefepime + Tigecycline | Ticarcillin tazobactam | No | Yes |
| 21 | 88 | M | Propionibacterium acnes | Negative | E. coli prostatitis and coma on epilepsy in the context of the antiepilepticus treatment interruption | Epilepsy benign prostatic hyperplasia | No | Yes | Yes | Amoxicillin + clavulanic acid | Ceftriaxone | No | Yes |
| 22 | 69 | M | S. aureus | Negative | Septic shock on the central catheter | Implantable defibrillator gastrostomy for swallowing disorder, multiple sclerosis | No s | Yes | Yes | Ceftriaxone + levofloxacin | Ticarcillin tazobactam + vancomycin | No | Yes |
| 23 | 49 | M | S. epidermidis | Negative | Septic shock complicated by renal failure and related to bacteremia with the implantable chamber | Bricker’s surgery at birth for congenital bladder atrophy, kidney transplant at age 37 years 2 years ago: colostomy for occlusive syndrome 1 month ago, complicated with removal of Bricker and nephrostomy | Yes | Yes | Yes | Cefepime + tigecycline | Tigecycline | No | Yes |
| 24 | 85 | F | S. aureus | Negative | S. aureus bacteremia on a venous catheter | Pulmonary arterial hypertension | No | Yes | Yes | Amoxicillin + Ticarcillin + tazobactam + Ceftriaxone | Ciprofloxacin | No | Yes |
| 25 | 81 | M | S. epidermidis | Negative | Influenza A and S. epidermidis bacteremia | Stage 4 right adrenal neuroblastoma with hepatic and bone involvement | No | Yes | Yes | Ceftriaxone | Vancomycin + Teicoplanin | No | Yes |
| 26 | 83 | F | S. epidermidis | Negative | Iron deficiency anemia with abdominal pain, fever 38°C, and vomiting; blood transfusion; fibroscopy: antral and fundic gastritis due to Helicobacter pylori, S. epidermidis bacteremia; ¼ blood culture | Pituitary macroadenoma complicated by insipidus diabetes osteosynthesis by centro medullary nail of the left femur 4 month ago | Yes | Yes | No | Ceftriaxone | Unchanged | No | Yes |
Abbreviations: F, female; M, male.
aAppropriate antibiotics refers to antibiotics known to exhibit an in vitro activity against M. smithii and prescribed prior to M. smithii detection in the blood.
Characteristics of 26 Patients Diagnosed With Methanobrevibacter smithii Archaemia
| Case | Age, y | Sex | Bacterial Culture | Methanobrevibacter smithii culture | Medical History | Risk Factor | Digestive Symptoms | Central Catheter | Previous Antibiotics | Previous Antibiotic Regimen | Second-line Antibiotics | Appropriate Antibiotica | Survived |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 60 | F | Staphylococcus hominis | Negative | Influenza B during a return to Mecca | None | Yes | No | No | Amoxicillin + clavulanic acid | No | Yes | |
| 2 | 45 | M | Streptococcus oralis | Negative | Central venous catheter infection | Lingual carcinoma chemotherapy and immunotherapy | No | Yes | No | Imipenem + linezolid | No | No; 4 months | |
| 3 | 44 | F | Streptococcus mutans | Positive | Infectious endocarditis on the native mitral valve | None | No | No | Yes | Vancomycin + gentamicin | Ceftriaxone + gentamycin | No | Yes |
| 4 | 60 | F | Klebsiella oxytoca | Negative | Septic shock and occlusive syndrome | Ovarian cancer in 2008 | Yes | Yes | Yes | Ceftriaxone metronidazole | Unchanged | Yes | Yes |
| 5 | 60 | M | S. hominis | Negative | Acute respiratory distress due to Streptococcus pneumoniae; left basal pneumonia | Chronic obstructive pulmonary disease | No | No | Yes | Cefotaxime | Unchanged | No | Yes |
| 6 | 78 | F | Escherichia coli | Negative | Obstructive pyelonephritis and septic shock | Bilateral breast cancer and metastatic colon cancer | No | Yes | Yes | Ticarcillin tazobactam | Imipenem | No | No. 1 day |
| 7 | 60 | M | Staphylococcus epidermidis | Positive | Infectious endocarditis on a mitral mechanical valve | Mitral mechanical; 1982 | Yes | No | Yes | Ofloxacin | Vancomycin + gentamycin | No | Yes |
| 8 | 57 | F | K. oxytoca | Negative | Progression of liver metastasis with febrile illness and abdominal pain | Carcinoid tumor of the small bowel with liver, pancreatic, bone, and mammary and lymph node metastases | No | Yes | No | Ticarcillin tazobactam | No | No. 2 days | |
| 9 | 55 | M | S. epidermidis | Negative | Epistaxis with thrombocytopenia, anemia, and fever on day 7 of chemotherapy and blood transfusion | Recurrence of Hodgkin’s lymphoma and chemotherapy | No | Yes | No | Ticarcillin tazobactam | No | Yes | |
| 10 | 59 | M | Actinomyces odontolyticus, Streptococcus anginosus | Negative | Septic shock secondary to hepatic abscess | Duodenal tumor treated by duodenopancreatectomy with choledocojejunal anastomosis in 2009 | Yes | No | No | Imipenem + gentamycin + vancomycin | No | Yes | |
| 11 | 80 | F | Staphylococcus aureus | Negative | Mitral native valve infective endocarditis complicated with aortic mycotic aneurysm of the renal aorta ruptured | Bilateral hip prosthesis, obesity, dysthyroidism | Yes | No | No | Oxacillin | No | No. 7 days | |
| 12 | 57 | M | Morganella morganii | Negative | Vascular surgery with iliofemoropopliteal bypass graft and cutaneous excision of skin lesion complicated with hemorrhage with blood transfusion | Right scarpa melanoma with vascular invasion | No | Yes | No | Cotrimoxazole | No | Yes | |
| 13 | 75 | F | S. hominis | Negative | Acute myeloblastic leukemia; fever after 24 hours of chemotherapy | Ovarian carcinoma in 2003 | No | Yes | Yes | Cotrimoxazole | Ticarcillin tazobactam | No | Yes |
| 14 | 72 | M | Enterobacter cloacae | Negative | Febrile occlusive syndrome due to the perforation of the posterior gastric wall involving a collection in the back cavity of the epiploons and a zone of renal parenchymal necrosis complicated with hemorrhage with blood transfusion | Attempted suicide by firearm, resulting in transfixing the gastric wound, hepatic wound, and retroperitoneal hematoma with hemorrhage | Yes | Yes | No | Ticarcillin tazobactam | No | Yes | |
| 15 | 71 | M | S. aureus | Negative | Nosocomial infection 3 weeks after neurosurgery for spinal arthrodesis for spondylodiscitis | Demyelinating Charcot-Marie-Tooth neuropathy | No | No | Yes | Vancomycin | Cotrimoxazole + clindamycin + Ofloxacin + rifampicin | Yes | Yes |
| 16 | 31 | M | S. epidermidis | Negative | High-speed road accident complicated by severe cranial tremor and the rupture of the aortic isthmus; fever and pneumonia 4 days after surgery | No | Yes | Yes | Amoxicillin + clavulanic acid | Cefepime | No | Yes | |
| 17 | 50 | F | Staphylococcus haemolyticus | Negative | Occlusive syndrome on peritoneal carcinoma surgery with lateral ileo-colic anastomosis central catheter ablation | Squamous cell carcinoma of the cervix with peritoneal metastases | Yes | Yes | No | Linezolid | No | Yes | |
| 18 | 2 | M | E. cloacae | Negative | Fever and septic shock | Liver transplant 8 months before for biliary atresia | No | Ye s | Yes | Ticarcillin tazobactam + Amikacin | Ticarcillin tazobactam + Amikacin | No | Yes |
| 19 | 50 | M | E. coli | Negative | Graft pyelonephritis urine culture E. coli | Kidney transplant for polycystic kidney disease 15 years earlier | No | No | Yes | Ceftriaxone + Ciprofloxacin | Ciprofloxacin | No | Yes |
| 20 | 38 | M | Bacteroides uniformis | Negative | Cephalic duodeno-pancreatectomy in the context of a neuroendocrine tumor complicated by hypovolemic shock, fever, splenic vein thrombosis, and small intestine necrosis; abdominal drainage culture: Enterococcus faecium, E. coli | Neuroendocrine tumor chemotherapy; biliary prosthesis 5 months before | Yes | Yes | Yes | Cefepime + Tigecycline | Ticarcillin tazobactam | No | Yes |
| 21 | 88 | M | Propionibacterium acnes | Negative | E. coli prostatitis and coma on epilepsy in the context of the antiepilepticus treatment interruption | Epilepsy benign prostatic hyperplasia | No | Yes | Yes | Amoxicillin + clavulanic acid | Ceftriaxone | No | Yes |
| 22 | 69 | M | S. aureus | Negative | Septic shock on the central catheter | Implantable defibrillator gastrostomy for swallowing disorder, multiple sclerosis | No s | Yes | Yes | Ceftriaxone + levofloxacin | Ticarcillin tazobactam + vancomycin | No | Yes |
| 23 | 49 | M | S. epidermidis | Negative | Septic shock complicated by renal failure and related to bacteremia with the implantable chamber | Bricker’s surgery at birth for congenital bladder atrophy, kidney transplant at age 37 years 2 years ago: colostomy for occlusive syndrome 1 month ago, complicated with removal of Bricker and nephrostomy | Yes | Yes | Yes | Cefepime + tigecycline | Tigecycline | No | Yes |
| 24 | 85 | F | S. aureus | Negative | S. aureus bacteremia on a venous catheter | Pulmonary arterial hypertension | No | Yes | Yes | Amoxicillin + Ticarcillin + tazobactam + Ceftriaxone | Ciprofloxacin | No | Yes |
| 25 | 81 | M | S. epidermidis | Negative | Influenza A and S. epidermidis bacteremia | Stage 4 right adrenal neuroblastoma with hepatic and bone involvement | No | Yes | Yes | Ceftriaxone | Vancomycin + Teicoplanin | No | Yes |
| 26 | 83 | F | S. epidermidis | Negative | Iron deficiency anemia with abdominal pain, fever 38°C, and vomiting; blood transfusion; fibroscopy: antral and fundic gastritis due to Helicobacter pylori, S. epidermidis bacteremia; ¼ blood culture | Pituitary macroadenoma complicated by insipidus diabetes osteosynthesis by centro medullary nail of the left femur 4 month ago | Yes | Yes | No | Ceftriaxone | Unchanged | No | Yes |
| Case | Age, y | Sex | Bacterial Culture | Methanobrevibacter smithii culture | Medical History | Risk Factor | Digestive Symptoms | Central Catheter | Previous Antibiotics | Previous Antibiotic Regimen | Second-line Antibiotics | Appropriate Antibiotica | Survived |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 60 | F | Staphylococcus hominis | Negative | Influenza B during a return to Mecca | None | Yes | No | No | Amoxicillin + clavulanic acid | No | Yes | |
| 2 | 45 | M | Streptococcus oralis | Negative | Central venous catheter infection | Lingual carcinoma chemotherapy and immunotherapy | No | Yes | No | Imipenem + linezolid | No | No; 4 months | |
| 3 | 44 | F | Streptococcus mutans | Positive | Infectious endocarditis on the native mitral valve | None | No | No | Yes | Vancomycin + gentamicin | Ceftriaxone + gentamycin | No | Yes |
| 4 | 60 | F | Klebsiella oxytoca | Negative | Septic shock and occlusive syndrome | Ovarian cancer in 2008 | Yes | Yes | Yes | Ceftriaxone metronidazole | Unchanged | Yes | Yes |
| 5 | 60 | M | S. hominis | Negative | Acute respiratory distress due to Streptococcus pneumoniae; left basal pneumonia | Chronic obstructive pulmonary disease | No | No | Yes | Cefotaxime | Unchanged | No | Yes |
| 6 | 78 | F | Escherichia coli | Negative | Obstructive pyelonephritis and septic shock | Bilateral breast cancer and metastatic colon cancer | No | Yes | Yes | Ticarcillin tazobactam | Imipenem | No | No. 1 day |
| 7 | 60 | M | Staphylococcus epidermidis | Positive | Infectious endocarditis on a mitral mechanical valve | Mitral mechanical; 1982 | Yes | No | Yes | Ofloxacin | Vancomycin + gentamycin | No | Yes |
| 8 | 57 | F | K. oxytoca | Negative | Progression of liver metastasis with febrile illness and abdominal pain | Carcinoid tumor of the small bowel with liver, pancreatic, bone, and mammary and lymph node metastases | No | Yes | No | Ticarcillin tazobactam | No | No. 2 days | |
| 9 | 55 | M | S. epidermidis | Negative | Epistaxis with thrombocytopenia, anemia, and fever on day 7 of chemotherapy and blood transfusion | Recurrence of Hodgkin’s lymphoma and chemotherapy | No | Yes | No | Ticarcillin tazobactam | No | Yes | |
| 10 | 59 | M | Actinomyces odontolyticus, Streptococcus anginosus | Negative | Septic shock secondary to hepatic abscess | Duodenal tumor treated by duodenopancreatectomy with choledocojejunal anastomosis in 2009 | Yes | No | No | Imipenem + gentamycin + vancomycin | No | Yes | |
| 11 | 80 | F | Staphylococcus aureus | Negative | Mitral native valve infective endocarditis complicated with aortic mycotic aneurysm of the renal aorta ruptured | Bilateral hip prosthesis, obesity, dysthyroidism | Yes | No | No | Oxacillin | No | No. 7 days | |
| 12 | 57 | M | Morganella morganii | Negative | Vascular surgery with iliofemoropopliteal bypass graft and cutaneous excision of skin lesion complicated with hemorrhage with blood transfusion | Right scarpa melanoma with vascular invasion | No | Yes | No | Cotrimoxazole | No | Yes | |
| 13 | 75 | F | S. hominis | Negative | Acute myeloblastic leukemia; fever after 24 hours of chemotherapy | Ovarian carcinoma in 2003 | No | Yes | Yes | Cotrimoxazole | Ticarcillin tazobactam | No | Yes |
| 14 | 72 | M | Enterobacter cloacae | Negative | Febrile occlusive syndrome due to the perforation of the posterior gastric wall involving a collection in the back cavity of the epiploons and a zone of renal parenchymal necrosis complicated with hemorrhage with blood transfusion | Attempted suicide by firearm, resulting in transfixing the gastric wound, hepatic wound, and retroperitoneal hematoma with hemorrhage | Yes | Yes | No | Ticarcillin tazobactam | No | Yes | |
| 15 | 71 | M | S. aureus | Negative | Nosocomial infection 3 weeks after neurosurgery for spinal arthrodesis for spondylodiscitis | Demyelinating Charcot-Marie-Tooth neuropathy | No | No | Yes | Vancomycin | Cotrimoxazole + clindamycin + Ofloxacin + rifampicin | Yes | Yes |
| 16 | 31 | M | S. epidermidis | Negative | High-speed road accident complicated by severe cranial tremor and the rupture of the aortic isthmus; fever and pneumonia 4 days after surgery | No | Yes | Yes | Amoxicillin + clavulanic acid | Cefepime | No | Yes | |
| 17 | 50 | F | Staphylococcus haemolyticus | Negative | Occlusive syndrome on peritoneal carcinoma surgery with lateral ileo-colic anastomosis central catheter ablation | Squamous cell carcinoma of the cervix with peritoneal metastases | Yes | Yes | No | Linezolid | No | Yes | |
| 18 | 2 | M | E. cloacae | Negative | Fever and septic shock | Liver transplant 8 months before for biliary atresia | No | Ye s | Yes | Ticarcillin tazobactam + Amikacin | Ticarcillin tazobactam + Amikacin | No | Yes |
| 19 | 50 | M | E. coli | Negative | Graft pyelonephritis urine culture E. coli | Kidney transplant for polycystic kidney disease 15 years earlier | No | No | Yes | Ceftriaxone + Ciprofloxacin | Ciprofloxacin | No | Yes |
| 20 | 38 | M | Bacteroides uniformis | Negative | Cephalic duodeno-pancreatectomy in the context of a neuroendocrine tumor complicated by hypovolemic shock, fever, splenic vein thrombosis, and small intestine necrosis; abdominal drainage culture: Enterococcus faecium, E. coli | Neuroendocrine tumor chemotherapy; biliary prosthesis 5 months before | Yes | Yes | Yes | Cefepime + Tigecycline | Ticarcillin tazobactam | No | Yes |
| 21 | 88 | M | Propionibacterium acnes | Negative | E. coli prostatitis and coma on epilepsy in the context of the antiepilepticus treatment interruption | Epilepsy benign prostatic hyperplasia | No | Yes | Yes | Amoxicillin + clavulanic acid | Ceftriaxone | No | Yes |
| 22 | 69 | M | S. aureus | Negative | Septic shock on the central catheter | Implantable defibrillator gastrostomy for swallowing disorder, multiple sclerosis | No s | Yes | Yes | Ceftriaxone + levofloxacin | Ticarcillin tazobactam + vancomycin | No | Yes |
| 23 | 49 | M | S. epidermidis | Negative | Septic shock complicated by renal failure and related to bacteremia with the implantable chamber | Bricker’s surgery at birth for congenital bladder atrophy, kidney transplant at age 37 years 2 years ago: colostomy for occlusive syndrome 1 month ago, complicated with removal of Bricker and nephrostomy | Yes | Yes | Yes | Cefepime + tigecycline | Tigecycline | No | Yes |
| 24 | 85 | F | S. aureus | Negative | S. aureus bacteremia on a venous catheter | Pulmonary arterial hypertension | No | Yes | Yes | Amoxicillin + Ticarcillin + tazobactam + Ceftriaxone | Ciprofloxacin | No | Yes |
| 25 | 81 | M | S. epidermidis | Negative | Influenza A and S. epidermidis bacteremia | Stage 4 right adrenal neuroblastoma with hepatic and bone involvement | No | Yes | Yes | Ceftriaxone | Vancomycin + Teicoplanin | No | Yes |
| 26 | 83 | F | S. epidermidis | Negative | Iron deficiency anemia with abdominal pain, fever 38°C, and vomiting; blood transfusion; fibroscopy: antral and fundic gastritis due to Helicobacter pylori, S. epidermidis bacteremia; ¼ blood culture | Pituitary macroadenoma complicated by insipidus diabetes osteosynthesis by centro medullary nail of the left femur 4 month ago | Yes | Yes | No | Ceftriaxone | Unchanged | No | Yes |
Abbreviations: F, female; M, male.
aAppropriate antibiotics refers to antibiotics known to exhibit an in vitro activity against M. smithii and prescribed prior to M. smithii detection in the blood.
M. smithii Culture and Genome Analysis
Methanobrevibacter smithii from 3 of the 16 PCR-positive anaerobic blood cultures grew in broth, and we were able to subculture M. smithii strain BC55 in case 3 and M. smithii strain BC84 in case 7, whereas subculture of the third strain on agar plate failed (Figure 3). Methanobrevibacter smithii strain BC55 exhibited a 1 712 416-bp genome, 1647 coding-gene chromosome of 31.3% G+C content; the respective figures for M. smithii strain BC84 were 1 720 237 bp, 1652, and 31.2%. A total of 32 transfer RNAs and 1 16S rRNA were identified in both isolates. The BC55 and BC84 strains differed by 75 single-nucleotide polymorphisms, belonged to the same M. smithii group (Supplementary Figure 3), and were most closely related to human feces isolates of the M. smithii strain DSM 2374 and the M. smithii strain C2_CSUR_P5 (CCXV01000001.1).
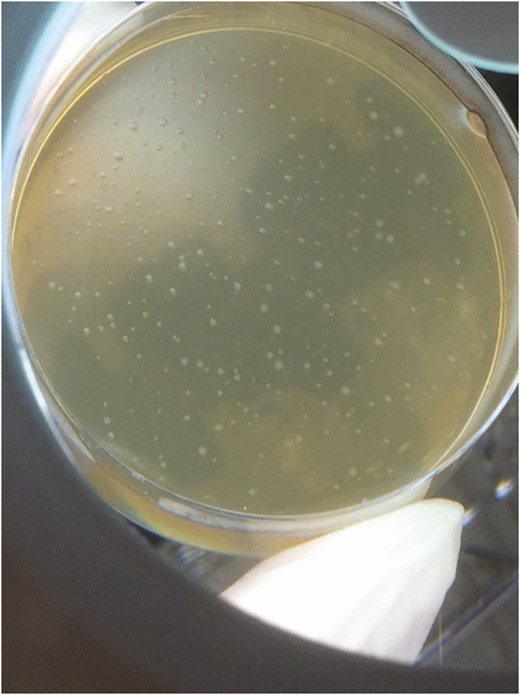
Methanobrevibacter smithii colonies were isolated via culture from the blood of a 60-year-old febrile male (patient 7).
DISCUSSION
In this work, we highlight the presence of M. smithii in the blood cultures of febrile patients. In 3 unrelated patients, the diagnosis was confirmed as M. smithii was isolated from 1 anaerobe blood culture and demonstrated by 2 microscopic methods and by 2 PCR-based methods in the cardiac tissues in 1 patient; M. smithii was isolated from the anaerobic blood culture in another patient; and M. smithii demonstrated by 2 microscopic methods and by 2 PCR-based methods in the vascular tissues in 1 patient. The 2 M. smithii isolates were genome-sequenced, which confirmed the identification and showed that both genomes were closely related but were distinct, ruling out contamination by previously known strains. The fact that in blood culture experimentally inoculated with bacteria alone (and in their negative controls), no methane and no M. smithii were detected, further indicating that the results reported here did not result from contamination or lack of specificity of the detection. Also, the measured prevalence of 0.5% of positive anaerobic blood cultures showed that this phenomenon is not uncommon, corresponding to 5 positive people per 100 000 inhabitants in the region where the study was conducted (Marseilles area of France).
Demonstration of M. smithii in the blood and tissues was surprising. Methanogens have thus far proven to be difficult to research in infectious diseases because of the difficulty in culturing these organisms, which requires both anaerobiosis and the presence of hydrogen. We found that methanogens are extremely sensitive to oxygen, and we therefore decided to perform the first sampling from the bottle for the PCR test in an anaerobic cabinet rather than in a standard hood after a 10-day postincubation of the anaerobic blood culture bottle at room temperature. Care should be taken to avoid any contact of blood bottles with the ambient atmosphere, as we observed an exquisite susceptibility of M. smithii to oxygen. This point is crucial for the recovery of methanogens from blood culture bottles. In addition, the thickness of the wall of methanogens leads to resistance to standard extraction, which is a prerequisite for PCR analysis, and to standard PCR investigation. Accordingly, we had to invent a specific DNA extraction protocol (above identified as method 2) and a specific real-time PCR amplification in order to confirm the presence of methanogen DNA in 2 of 3 cardiac/vascular tissues investigated. The difficulties we encountered may be linked to the presence of PCR inhibitors in these samples and to the patchy nature of infection.
We detected M. smithii archaemia in ill, febrile patients in association with bacteria anaerobically cultured, which is characteristic of methanogens. In this study, M. smithii was the sole methanogen detected in blood, mirroring the fact that it is the methanogen most frequently encountered in the digestive microbiota [3] as well as in milk [15]. Here, its codetection with Enterobacteriaceae, which are likely to produce hydrogen [28, 29], was not surprising and could result from translocation; genomic data favor this hypothesis. The codetection of methanogens with staphylococci and streptococci was unexpected, as we confirmed that streptococci are not producing hydrogen contrary to some staphylococci. Staphylococci and streptococci produce formate [30, 31], which can be metabolized by M. smithii instead of hydrogen as an electron source for reducing carbon dioxide to methane [32]. Also, the fact that the majority of patients did not receive rifampicin or metronidazole, the sole antibiotics to be effective in vitro against methanogens [33], may have contributed to the detection of M. smithii in the blood. Codetection of methanogens with anaerobes as previously observed in life-threatening situations such as brain abscesses [10], raises the question of their relative role in infections. Currently, we are not able to determine the importance of methanogens in human pathology.
Overall, the tools developed here highlight the existence of methanogens in bacteremia, create a new field of human microbial pathology, and encourage systematic research to discover the role of methanogens, the prognosis of diseases associated with these microorganisms, and treatment strategies. In practice, the acknowledgment of the pathological role of methanogens is new. After describing their presence in brain abscesses, muscle abscesses, milk, most mucous membranes, and urinary tract infections [13], it is now necessary to develop strategies for their detection in most pathological situations, including those in which a bacterium has already been identified.
Supplementary Data
Supplementary materials are available at Clinical Infectious Diseases online. Consisting of data provided by the authors to benefit the reader, the posted materials are not copyedited and are the sole responsibility of the authors, so questions or comments should be addressed to the corresponding author.
Notes
Acknowledgments. The authors thank S. Taku, T. Irie, K. Imai, S. Matsubara, A. Hisada, and all Hitachi team members in Japan for the collaborative study with Hitachi High Technology and Institut Hospitalier Universitaire and for the installation of and service of the TM4000 microscope in our facility. The authors acknowledge Prof Hubert Lepidi for pathology examinations.
Financial support. This work was supported by the French Government under the Investissements d’avenir (Investments for the Future) program managed by the Agence Nationale de la Recherche (National Agency for Research; reference: Méditerranée Infection 10-IAHU-03). This work was supported by Région Sud (Provence Alpes Côte d’Azur) and European funding Fonds Européen de Développement Régional (FEDER) Plateformes de Recherche et d’Innovation Mutualisées Méditerranée Infection (PRIMMI).
Potential conflicts of interest. The authors: No reported conflicts of interest. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}