






Abstract
Since the introduction of Haemophilus influenzae serotype b (Hib) conjugate vaccines in the United States, invasive H. influenzae disease epidemiology has changed, and racial disparities have not been recently described.
Active population- and laboratory-based surveillance for H. influenzae was conducted through Active Bacterial Core surveillance at 10 US sites. Data from 2008–2017 were used to estimate projected nationwide annual incidence, as cases per 100 000.
During 2008–2017, Active Bacterial Core surveillance identified 7379 H. influenzae cases. Of 6705 patients (90.9%) with reported race, 76.2% were White, 18.6% were Black, 2.8% were Asian/Pacific Islander, and 2.4% were American Indian or Alaska Native (AI/AN). The nationwide annual incidence was 1.8 cases/100 000. By race, incidence was highest among AI/AN populations (3.1) and lowest among Asian/Pacific Islander populations (0.8). Nontypeable H. influenzae caused the largest incidence within all races (1.3), with no striking disparities identified. Among AI/AN children aged <5 years, incidence of H. influenzae serotype a (Hia) was 16.7 times higher and Hib incidence was 22.4 times higher than among White children. Although Hia incidence was lower among White and Black populations than among AI/AN populations, Hia incidence increased 13.6% annually among White children and 40.4% annually among Black children aged <5 years.
While nontypeable H. influenzae causes the largest H. influenzae burden overall, AI/AN populations experience disproportionately high rates of Hia and Hib, with the greatest disparity among AI/AN children aged <5 years. Prevention tools are needed to reduce disparities affecting AI/AN children and address increasing Hia incidence in other communities.
Haemophilus influenzae is an important bacterial cause of invasive disease (eg, meningitis and bacteremia) and noninvasive disease (eg, otitis media and sinusitis) in young children, older adults, and persons with certain medical conditions [1–3]. Both encapsulated (H. influenzae serotypes a [Hia], b [Hib], c [Hic], d [Hid], e [Hie], and f [Hif]) and unencapsulated (nontypeable H. influenzae [NTHi]) strains can cause infection.
Historically, Hib was the most common cause of invasive bacterial disease in children aged <5 years in the United States [4]. In the pre-Hib vaccine era, racial disparities in Hib disease were reported with incidence rates 3–4 times higher among Black children than among White children [5–10]. American Indian and Alaska Native (AI/AN) children experienced greater disparities, with an incidence of invasive Hib disease 5–10 times that among White children [11–13]. Among all ages, Black populations had invasive H. influenzae disease incidence 1.5–3.5 times higher than White populations [4, 7, 14].
After the introduction of Hib conjugate vaccine into the childhood immunization schedule during the 1980s and 1990s, the incidence of Hib disease in children aged <5 years declined dramatically among all racial groups [15, 16]. Since then, H. influenzae disease epidemiology has changed. NTHi currently accounts for >70% of invasive H. influenzae disease cases [3]. In addition, from 2002 to 2015, the incidences of Hia and NTHi increased annually by 13% and 3%, respectively [3].
With this changing epidemiology, it is important to monitor whether racial disparities in invasive H. influenzae disease persist. We analyzed data from active population- and laboratory-based surveillance for 2008–2017 to identify current racial disparities in invasive H. influenzae disease in the United States and to help inform the design and implementation of prevention strategies.
METHODS
Surveillance
Invasive H. influenzae disease data were collected through Active Bacterial Core surveillance (ABCs), an active population- and laboratory-based surveillance system supported by the Centers for Disease Control and Prevention (CDC) as a part of the Emerging Infections Program [17]. Data from 2008 through 2017 were included in the analysis.
The surveillance areas included California (3 San Francisco Bay–area counties), Colorado (5 Denver-area counties), Connecticut (statewide), Georgia (20 Atlanta-area counties, 2008–2009; statewide, 2010–2017), Maryland (statewide), Minnesota (statewide), New Mexico (statewide), New York (15 Rochester- and Albany-area counties), Oregon (statewide), and Tennessee (11 counties, 2008–2009; 20 counties, 2010–2017). The population under surveillance represented 11.9% of the US population in 2008 and 13.7% in 2017 [18]. Race was classified as White, Black, Asian/Pacific Islander (PI), or AI/AN. The racial distribution of the population under ABCs was 77.1% White, 15.8% Black, 5.8% Asian/PI, and 1.3% AI/AN in 2008, and 73.0% White, 18.4% Black, 7.1% Asian/PI, and 1.5% AI/AN in 2017.
A case of invasive H. influenzae disease was defined as isolation of H. influenzae from a normally sterile site (eg, blood, pleural fluid, and cerebrospinal fluid) in a surveillance-area resident. Epidemiologic and clinical information was abstracted from medical records. Infants with a gestational age ≤22 weeks were excluded. Outcome (alive or dead) was based on patient status at hospital discharge. A hierarchical definition was used to assign a single syndrome for cases: meningitis if a clinical diagnosis of meningitis was recorded in the medical record and H. influenzae was isolated from cerebrospinal fluid or other sterile sites, bacteremic pneumonia if pneumonia was recorded in the medical record and H. influenzae was isolated from blood or pleural fluid, and primary bacteremia if H. influenzae was isolated from blood and the medical record did not note another clinical syndrome. All other clinical syndromes were classified based on source of isolate or information noted in the medical record.
Vaccination histories of children aged <5 years with Hib disease were abstracted from medical records and state vaccine registries. Children were considered age-appropriately vaccinated or fully vaccinated if vaccinated according to the recommended schedule for age and vaccine product [19]. Children who received ≥1 dose of Hib vaccine but not all recommended doses for their age and vaccine product were considered undervaccinated. Children were considered unvaccinated if they had not received any Hib vaccine doses and were aged >2 months. Children aged ≤2 months were considered too young to receive vaccine. Vaccine type is reported as Hib antigen polyribosylribitol phosphate (PRP) conjugated to either meningococcal outer membrane protein (OMP), tetanus toxoid (T), or mutant diphtheria toxin CRM197 (CRM).
Laboratory Methods
State public health laboratories serotyped and sent H. influenzae isolates to CDC’s Bacterial Meningitis Laboratory, where species and serotyping were confirmed for all isolates by means of real-time polymerase chain reaction and/or slide agglutination [3, 20, 21].
Statistical Analysis
Case fatality ratios were calculated using the proportion of cases with known outcomes as the denominator. Kruskal-Wallis tests were used to compare medians of continuous variables. Pearson χ 2 and Fisher exact tests were used to compare categorical variables. For the ABCs sites, incidence rates were reported as cases per 100 000 and calculated using National Center for Health Statistics bridged-race postcensal population estimates [18]; nationwide estimates were calculated by direct standardization to the age and race distribution of the US population. For race-stratified nationwide incidence estimates, missing race was multiply imputed using sequential regression multiple imputation [22]. Multiply imputed data sets were created using IVEware software Version 0.3 (Institute for Social Research, University of Michigan, Ann Arbor).
Variance estimates were calculated using standard combining rules for multiply imputed data. The 95% confidence intervals (CIs) around the directly standardized incidences were calculated using a method derived from the relationship between the Poisson distribution and the gamma distribution, whereas estimated age-, race-, and serotype-specific 95% CIs were calculated using exact CIs for a Poisson random variable [23]. Incidences in Black, Asian/PI, and AI/AN populations were compared with those in White populations, and incidence rate ratios (IRRs) were calculated. A negative binomial model was used to estimate annual percentage changes in incidence.
This project was reviewed in accordance with CDC human research protection procedures and was determined to be nonresearch public health surveillance. At each ABCs site, it was deemed either a public health assessment or human subjects research, for which approval was granted by local institutional review boards.
RESULTS
Patient Characteristics
From 2008 to 2017, a total of 7379 cases of invasive H. influenzae disease were reported from ABCs sites. Patient race was reported in 6705 cases (90.9%); of these patients, 76.2% were White, 18.6% were Black, 2.8% were Asian/PI, and 2.4% were AI/AN (Table 1). The median age was 68 years for White, 50 years for Black, 61 years for Asian/PI, and 24 years for AI/AN patients (P < .001). While children aged <5 years accounted for <20% of cases in White, Black, and Asian/PI patients, they represented almost half (46.6%) of cases in AI/AN patients.
Epidemiologic and Clinical Characteristics of Patients With Invasive Haemophilus influenzae Disease, by Race—Active Bacterial Core Surveillance, 2008–2017
| Patients, No. (%)a | |||||
|---|---|---|---|---|---|
| Characteristic | White | Black | Asian/PI | AI/AN | All Races |
| All patients | 5106 (76.2) | 1248 (18.6) | 190 (2.8) | 161 (2.4) | 6705 (100) |
| Age, median (IQR), y | 68 (52–81) | 50 (23–65) | 61 (25–78) | 24 (1–60) | 64 (44–79) |
| Age <5 y | 443 (8.7) | 212 (17.0) | 32 (16.8) | 75 (46.6) | 762 (11.4) |
| Sex | |||||
| Male | 2334 (45.7) | 552 (44.2) | 95 (50.0) | 78 (48.5) | 3059 (45.6) |
| Female | 2772 (54.3) | 696 (55.8) | 95 (50.0) | 83 (51.6) | 3646 (54.4) |
| Ethnicity | |||||
| Hispanic | 236 (4.6) | 13 (1.0) | 9 (4.7) | 8 (5.0) | 266 (4.0) |
| Non-Hispanic | 3679 (72.1) | 950 (76.1) | 160 (84.2) | 111 (68.9) | 4900 (73.1) |
| Unknown | 1191 (23.3) | 285 (22.8) | 21 (11.1) | 42 (26.1) | 1539 (23.0) |
| Serotypeb | |||||
| NTHi | 3371 (73.5) | 750 (67.8) | 135 (82.3) | 56 (37.1) | 4312 (71.8) |
| Hia | 230 (5.0) | 57 (5.2) | 5 (3.1) | 57 (37.8) | 349 (5.8) |
| Hib | 70 (1.5) | 14 (1.3) | 3 (1.8) | 20 (13.3) | 107 (1.8) |
| Hic | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.7) | 1 (0.0) |
| Hid | 2 (0.0) | 2 (0.2) | 0 (0.0) | 0 (0.0) | 4 (0.1) |
| Hie | 220 (4.8) | 53 (4.8) | 3 (1.8) | 4 (2.7) | 280 (4.7) |
| Hif | 692 (15.1) | 231 (20.9) | 18 (11.0) | 13 (8.6) | 954 (15.9) |
| Clinical syndromec | |||||
| Bacteremic pneumonia | 3079 (60.7) | 575 (46.5) | 94 (50.3) | 67 (41.9) | 3815 (57.3) |
| Bacteremia | 1506 (29.7) | 496 (40.1) | 73 (39.0) | 51 (31.9) | 2126 (31.9) |
| Meningitis | 327 (6.4) | 91 (7.4) | 4 (2.1) | 34 (21.3) | 456 (6.9) |
| Other | 160 (3.2) | 74 (6.0) | 16 (8.6) | 8 (5.0) | 258 (3.9) |
| Hospitalizedd | 4789 (94.1) | 1129 (90.7) | 182 (95.8) | 147 (91.9) | 6274 (93.9) |
| Case fatality ratioe | 738 (14.6) | 142 (11.5) | 23 (12.2) | 23 (14.3) | 926 (13.9) |
| Patients, No. (%)a | |||||
|---|---|---|---|---|---|
| Characteristic | White | Black | Asian/PI | AI/AN | All Races |
| All patients | 5106 (76.2) | 1248 (18.6) | 190 (2.8) | 161 (2.4) | 6705 (100) |
| Age, median (IQR), y | 68 (52–81) | 50 (23–65) | 61 (25–78) | 24 (1–60) | 64 (44–79) |
| Age <5 y | 443 (8.7) | 212 (17.0) | 32 (16.8) | 75 (46.6) | 762 (11.4) |
| Sex | |||||
| Male | 2334 (45.7) | 552 (44.2) | 95 (50.0) | 78 (48.5) | 3059 (45.6) |
| Female | 2772 (54.3) | 696 (55.8) | 95 (50.0) | 83 (51.6) | 3646 (54.4) |
| Ethnicity | |||||
| Hispanic | 236 (4.6) | 13 (1.0) | 9 (4.7) | 8 (5.0) | 266 (4.0) |
| Non-Hispanic | 3679 (72.1) | 950 (76.1) | 160 (84.2) | 111 (68.9) | 4900 (73.1) |
| Unknown | 1191 (23.3) | 285 (22.8) | 21 (11.1) | 42 (26.1) | 1539 (23.0) |
| Serotypeb | |||||
| NTHi | 3371 (73.5) | 750 (67.8) | 135 (82.3) | 56 (37.1) | 4312 (71.8) |
| Hia | 230 (5.0) | 57 (5.2) | 5 (3.1) | 57 (37.8) | 349 (5.8) |
| Hib | 70 (1.5) | 14 (1.3) | 3 (1.8) | 20 (13.3) | 107 (1.8) |
| Hic | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.7) | 1 (0.0) |
| Hid | 2 (0.0) | 2 (0.2) | 0 (0.0) | 0 (0.0) | 4 (0.1) |
| Hie | 220 (4.8) | 53 (4.8) | 3 (1.8) | 4 (2.7) | 280 (4.7) |
| Hif | 692 (15.1) | 231 (20.9) | 18 (11.0) | 13 (8.6) | 954 (15.9) |
| Clinical syndromec | |||||
| Bacteremic pneumonia | 3079 (60.7) | 575 (46.5) | 94 (50.3) | 67 (41.9) | 3815 (57.3) |
| Bacteremia | 1506 (29.7) | 496 (40.1) | 73 (39.0) | 51 (31.9) | 2126 (31.9) |
| Meningitis | 327 (6.4) | 91 (7.4) | 4 (2.1) | 34 (21.3) | 456 (6.9) |
| Other | 160 (3.2) | 74 (6.0) | 16 (8.6) | 8 (5.0) | 258 (3.9) |
| Hospitalizedd | 4789 (94.1) | 1129 (90.7) | 182 (95.8) | 147 (91.9) | 6274 (93.9) |
| Case fatality ratioe | 738 (14.6) | 142 (11.5) | 23 (12.2) | 23 (14.3) | 926 (13.9) |
Abbreviations: AI/AN, American Indian or Alaska Native; Hia, Haemophilus influenzae serotype a; Hib, H. influenzae serotype b; Hic, H. influenzae serotype c; Hid, H. influenzae serotype d; Hie, H. influenzae serotype e; Hif, H. influenzae serotype f; IQR, interquartile range; NTHi, nontypeable H influenzae; PI, Pacific Islander.
aData represent no. (%) of patients unless otherwise specified. Patients with unknown race (n = 674 [9.1%]) are excluded.
bAmong patients with known serotype (n = 6007 [89.6%]).
cAmong patients with known syndrome (n = 6655 [99.3%]).
dAmong patients with known hospitalization status (n = 6683 [99.7%]).
eAmong patients with known outcome (n = 6652 [99.2%]).
Epidemiologic and Clinical Characteristics of Patients With Invasive Haemophilus influenzae Disease, by Race—Active Bacterial Core Surveillance, 2008–2017
| Patients, No. (%)a | |||||
|---|---|---|---|---|---|
| Characteristic | White | Black | Asian/PI | AI/AN | All Races |
| All patients | 5106 (76.2) | 1248 (18.6) | 190 (2.8) | 161 (2.4) | 6705 (100) |
| Age, median (IQR), y | 68 (52–81) | 50 (23–65) | 61 (25–78) | 24 (1–60) | 64 (44–79) |
| Age <5 y | 443 (8.7) | 212 (17.0) | 32 (16.8) | 75 (46.6) | 762 (11.4) |
| Sex | |||||
| Male | 2334 (45.7) | 552 (44.2) | 95 (50.0) | 78 (48.5) | 3059 (45.6) |
| Female | 2772 (54.3) | 696 (55.8) | 95 (50.0) | 83 (51.6) | 3646 (54.4) |
| Ethnicity | |||||
| Hispanic | 236 (4.6) | 13 (1.0) | 9 (4.7) | 8 (5.0) | 266 (4.0) |
| Non-Hispanic | 3679 (72.1) | 950 (76.1) | 160 (84.2) | 111 (68.9) | 4900 (73.1) |
| Unknown | 1191 (23.3) | 285 (22.8) | 21 (11.1) | 42 (26.1) | 1539 (23.0) |
| Serotypeb | |||||
| NTHi | 3371 (73.5) | 750 (67.8) | 135 (82.3) | 56 (37.1) | 4312 (71.8) |
| Hia | 230 (5.0) | 57 (5.2) | 5 (3.1) | 57 (37.8) | 349 (5.8) |
| Hib | 70 (1.5) | 14 (1.3) | 3 (1.8) | 20 (13.3) | 107 (1.8) |
| Hic | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.7) | 1 (0.0) |
| Hid | 2 (0.0) | 2 (0.2) | 0 (0.0) | 0 (0.0) | 4 (0.1) |
| Hie | 220 (4.8) | 53 (4.8) | 3 (1.8) | 4 (2.7) | 280 (4.7) |
| Hif | 692 (15.1) | 231 (20.9) | 18 (11.0) | 13 (8.6) | 954 (15.9) |
| Clinical syndromec | |||||
| Bacteremic pneumonia | 3079 (60.7) | 575 (46.5) | 94 (50.3) | 67 (41.9) | 3815 (57.3) |
| Bacteremia | 1506 (29.7) | 496 (40.1) | 73 (39.0) | 51 (31.9) | 2126 (31.9) |
| Meningitis | 327 (6.4) | 91 (7.4) | 4 (2.1) | 34 (21.3) | 456 (6.9) |
| Other | 160 (3.2) | 74 (6.0) | 16 (8.6) | 8 (5.0) | 258 (3.9) |
| Hospitalizedd | 4789 (94.1) | 1129 (90.7) | 182 (95.8) | 147 (91.9) | 6274 (93.9) |
| Case fatality ratioe | 738 (14.6) | 142 (11.5) | 23 (12.2) | 23 (14.3) | 926 (13.9) |
| Patients, No. (%)a | |||||
|---|---|---|---|---|---|
| Characteristic | White | Black | Asian/PI | AI/AN | All Races |
| All patients | 5106 (76.2) | 1248 (18.6) | 190 (2.8) | 161 (2.4) | 6705 (100) |
| Age, median (IQR), y | 68 (52–81) | 50 (23–65) | 61 (25–78) | 24 (1–60) | 64 (44–79) |
| Age <5 y | 443 (8.7) | 212 (17.0) | 32 (16.8) | 75 (46.6) | 762 (11.4) |
| Sex | |||||
| Male | 2334 (45.7) | 552 (44.2) | 95 (50.0) | 78 (48.5) | 3059 (45.6) |
| Female | 2772 (54.3) | 696 (55.8) | 95 (50.0) | 83 (51.6) | 3646 (54.4) |
| Ethnicity | |||||
| Hispanic | 236 (4.6) | 13 (1.0) | 9 (4.7) | 8 (5.0) | 266 (4.0) |
| Non-Hispanic | 3679 (72.1) | 950 (76.1) | 160 (84.2) | 111 (68.9) | 4900 (73.1) |
| Unknown | 1191 (23.3) | 285 (22.8) | 21 (11.1) | 42 (26.1) | 1539 (23.0) |
| Serotypeb | |||||
| NTHi | 3371 (73.5) | 750 (67.8) | 135 (82.3) | 56 (37.1) | 4312 (71.8) |
| Hia | 230 (5.0) | 57 (5.2) | 5 (3.1) | 57 (37.8) | 349 (5.8) |
| Hib | 70 (1.5) | 14 (1.3) | 3 (1.8) | 20 (13.3) | 107 (1.8) |
| Hic | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.7) | 1 (0.0) |
| Hid | 2 (0.0) | 2 (0.2) | 0 (0.0) | 0 (0.0) | 4 (0.1) |
| Hie | 220 (4.8) | 53 (4.8) | 3 (1.8) | 4 (2.7) | 280 (4.7) |
| Hif | 692 (15.1) | 231 (20.9) | 18 (11.0) | 13 (8.6) | 954 (15.9) |
| Clinical syndromec | |||||
| Bacteremic pneumonia | 3079 (60.7) | 575 (46.5) | 94 (50.3) | 67 (41.9) | 3815 (57.3) |
| Bacteremia | 1506 (29.7) | 496 (40.1) | 73 (39.0) | 51 (31.9) | 2126 (31.9) |
| Meningitis | 327 (6.4) | 91 (7.4) | 4 (2.1) | 34 (21.3) | 456 (6.9) |
| Other | 160 (3.2) | 74 (6.0) | 16 (8.6) | 8 (5.0) | 258 (3.9) |
| Hospitalizedd | 4789 (94.1) | 1129 (90.7) | 182 (95.8) | 147 (91.9) | 6274 (93.9) |
| Case fatality ratioe | 738 (14.6) | 142 (11.5) | 23 (12.2) | 23 (14.3) | 926 (13.9) |
Abbreviations: AI/AN, American Indian or Alaska Native; Hia, Haemophilus influenzae serotype a; Hib, H. influenzae serotype b; Hic, H. influenzae serotype c; Hid, H. influenzae serotype d; Hie, H. influenzae serotype e; Hif, H. influenzae serotype f; IQR, interquartile range; NTHi, nontypeable H influenzae; PI, Pacific Islander.
aData represent no. (%) of patients unless otherwise specified. Patients with unknown race (n = 674 [9.1%]) are excluded.
bAmong patients with known serotype (n = 6007 [89.6%]).
cAmong patients with known syndrome (n = 6655 [99.3%]).
dAmong patients with known hospitalization status (n = 6683 [99.7%]).
eAmong patients with known outcome (n = 6652 [99.2%]).
Among 6007 reported cases (89.6%) with serotyping data available, 71.8% were NTHi, 5.8% Hia, 1.8% Hib, 0.0% Hic, 0.1% Hid, 4.7% Hie, and 15.9% Hif (Table 1). NTHi was the predominant cause of invasive H. influenzae among White (73.5%), Black (67.8%), and Asian/PI (82.3%) patients. By contrast, NTHi (37.1%) and Hia (37.8%) predominated among AI/AN patients. Although Hib caused <2% of H. influenzae cases among White, Black, and Asian/PI patients, it caused significantly more H. influenzae disease in AI/AN patients (13.3%; P < .001). Bacteremic pneumonia was the most common clinical syndrome among all races (57.3%; Table 1). A larger proportion of cases among AI/AN patients presented as meningitis (21.3%). Case fatality ratios ranged from 11.5% in Black patients to 14.6% in White patients.
Incidence Trends
From 2008 to 2017, the average annual incidence of invasive H. influenzae disease was 1.8 cases/100 000 (Table 2). By race, incidence was highest among AI/AN populations (3.1 cases/100 000) and lowest among Asian/PI populations (0.8 cases/100 000). The incidences among White and Black populations were similar: 1.8 and 1.9 cases/100 000, respectively. AI/AN populations had the highest incidence throughout most of the analysis period (2008–2016; Figure 1), although the incidence declined by 2.2% annually (95% CI, −4.0% to −.3%) overall. During this period, incidences increased 3.9% annually (95% CI, 3.6%–4.2%) in White populations, 3.7% annually (2.9%–4.5%) in Black populations, and 3.0% annually (1.1%–4.8%) in Asian/PI populations.
Estimated Average Annual Incidence of Invasive Haemophilus influenzae Disease, by Age Group and Race—United States, 2008–2017
| White | Black | Asian/PI | AI/AN | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Age, y | Incidencea | IRR | Incidencea | IRR (95% CI) | Incidencea | IRR (95% CI) | Incidencea | IRR (95% CI) | Total Incidencea |
| <1 | 8.0 | Ref | 11.2 | 1.4 (1.1–1.7) | 5.7 | 0.7 (.4–1.2) | 34.9 | 4.4 (3.1–6.2) | 8.9 |
| 1–4 | 1.2 | Ref | 2.3 | 1.9 (1.5–2.4) | 1.1 | 0.9 (.6–1.6) | 8.8 | 7.1 (5.0–10.0) | 1.6 |
| 5–17 | 0.3 | Ref | 0.5 | 1.6 (1.2–2.1) | 0.3 | 0.8 (.4–1.5) | 0.3 | 0.9 (.3–2.6) | 0.4 |
| 18–34 | 0.4 | Ref | 0.9 | 2.3 (1.9–2.8) | 0.2 | 0.6 (.4–1.1) | 0.8 | 2.2 (1.2–4.0) | 0.5 |
| 35–49 | 0.7 | Ref | 1.3 | 2.0 (1.7–2.4) | 0.4 | 0.6 (.4–1.0) | 1.9 | 3.0 (1.9–4.7) | 0.7 |
| 50–64 | 1.8 | Ref | 2.6 | 1.5 (1.3–1.7) | 0.8 | 0.4 (.3–.6) | 3.5 | 2.0 (1.4–2.9) | 1.8 |
| ≥65 | 6.8 | Ref | 5.6 | 0.8 (.7–.9) | 3.5 | 0.5 (.4–.7) | 9.4 | 1.4 (1.0–2.0) | 6.6 |
| Total | 1.8 | Ref | 1.9 | 1.0 (1.0–1.1) | 0.8 | 0.4 (.4–.5) | 3.1 | 1.7 (1.5–2.0) | 1.8 |
| White | Black | Asian/PI | AI/AN | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Age, y | Incidencea | IRR | Incidencea | IRR (95% CI) | Incidencea | IRR (95% CI) | Incidencea | IRR (95% CI) | Total Incidencea |
| <1 | 8.0 | Ref | 11.2 | 1.4 (1.1–1.7) | 5.7 | 0.7 (.4–1.2) | 34.9 | 4.4 (3.1–6.2) | 8.9 |
| 1–4 | 1.2 | Ref | 2.3 | 1.9 (1.5–2.4) | 1.1 | 0.9 (.6–1.6) | 8.8 | 7.1 (5.0–10.0) | 1.6 |
| 5–17 | 0.3 | Ref | 0.5 | 1.6 (1.2–2.1) | 0.3 | 0.8 (.4–1.5) | 0.3 | 0.9 (.3–2.6) | 0.4 |
| 18–34 | 0.4 | Ref | 0.9 | 2.3 (1.9–2.8) | 0.2 | 0.6 (.4–1.1) | 0.8 | 2.2 (1.2–4.0) | 0.5 |
| 35–49 | 0.7 | Ref | 1.3 | 2.0 (1.7–2.4) | 0.4 | 0.6 (.4–1.0) | 1.9 | 3.0 (1.9–4.7) | 0.7 |
| 50–64 | 1.8 | Ref | 2.6 | 1.5 (1.3–1.7) | 0.8 | 0.4 (.3–.6) | 3.5 | 2.0 (1.4–2.9) | 1.8 |
| ≥65 | 6.8 | Ref | 5.6 | 0.8 (.7–.9) | 3.5 | 0.5 (.4–.7) | 9.4 | 1.4 (1.0–2.0) | 6.6 |
| Total | 1.8 | Ref | 1.9 | 1.0 (1.0–1.1) | 0.8 | 0.4 (.4–.5) | 3.1 | 1.7 (1.5–2.0) | 1.8 |
Abbreviations: AI/AN, American Indian or Alaska Native; CI, confidence interval; IRR, incidence rate ratio; PI, Pacific Islander; Ref, reference category for IRR calculation.
aIncidence given as cases per 100 000 persons per year.
Estimated Average Annual Incidence of Invasive Haemophilus influenzae Disease, by Age Group and Race—United States, 2008–2017
| White | Black | Asian/PI | AI/AN | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Age, y | Incidencea | IRR | Incidencea | IRR (95% CI) | Incidencea | IRR (95% CI) | Incidencea | IRR (95% CI) | Total Incidencea |
| <1 | 8.0 | Ref | 11.2 | 1.4 (1.1–1.7) | 5.7 | 0.7 (.4–1.2) | 34.9 | 4.4 (3.1–6.2) | 8.9 |
| 1–4 | 1.2 | Ref | 2.3 | 1.9 (1.5–2.4) | 1.1 | 0.9 (.6–1.6) | 8.8 | 7.1 (5.0–10.0) | 1.6 |
| 5–17 | 0.3 | Ref | 0.5 | 1.6 (1.2–2.1) | 0.3 | 0.8 (.4–1.5) | 0.3 | 0.9 (.3–2.6) | 0.4 |
| 18–34 | 0.4 | Ref | 0.9 | 2.3 (1.9–2.8) | 0.2 | 0.6 (.4–1.1) | 0.8 | 2.2 (1.2–4.0) | 0.5 |
| 35–49 | 0.7 | Ref | 1.3 | 2.0 (1.7–2.4) | 0.4 | 0.6 (.4–1.0) | 1.9 | 3.0 (1.9–4.7) | 0.7 |
| 50–64 | 1.8 | Ref | 2.6 | 1.5 (1.3–1.7) | 0.8 | 0.4 (.3–.6) | 3.5 | 2.0 (1.4–2.9) | 1.8 |
| ≥65 | 6.8 | Ref | 5.6 | 0.8 (.7–.9) | 3.5 | 0.5 (.4–.7) | 9.4 | 1.4 (1.0–2.0) | 6.6 |
| Total | 1.8 | Ref | 1.9 | 1.0 (1.0–1.1) | 0.8 | 0.4 (.4–.5) | 3.1 | 1.7 (1.5–2.0) | 1.8 |
| White | Black | Asian/PI | AI/AN | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Age, y | Incidencea | IRR | Incidencea | IRR (95% CI) | Incidencea | IRR (95% CI) | Incidencea | IRR (95% CI) | Total Incidencea |
| <1 | 8.0 | Ref | 11.2 | 1.4 (1.1–1.7) | 5.7 | 0.7 (.4–1.2) | 34.9 | 4.4 (3.1–6.2) | 8.9 |
| 1–4 | 1.2 | Ref | 2.3 | 1.9 (1.5–2.4) | 1.1 | 0.9 (.6–1.6) | 8.8 | 7.1 (5.0–10.0) | 1.6 |
| 5–17 | 0.3 | Ref | 0.5 | 1.6 (1.2–2.1) | 0.3 | 0.8 (.4–1.5) | 0.3 | 0.9 (.3–2.6) | 0.4 |
| 18–34 | 0.4 | Ref | 0.9 | 2.3 (1.9–2.8) | 0.2 | 0.6 (.4–1.1) | 0.8 | 2.2 (1.2–4.0) | 0.5 |
| 35–49 | 0.7 | Ref | 1.3 | 2.0 (1.7–2.4) | 0.4 | 0.6 (.4–1.0) | 1.9 | 3.0 (1.9–4.7) | 0.7 |
| 50–64 | 1.8 | Ref | 2.6 | 1.5 (1.3–1.7) | 0.8 | 0.4 (.3–.6) | 3.5 | 2.0 (1.4–2.9) | 1.8 |
| ≥65 | 6.8 | Ref | 5.6 | 0.8 (.7–.9) | 3.5 | 0.5 (.4–.7) | 9.4 | 1.4 (1.0–2.0) | 6.6 |
| Total | 1.8 | Ref | 1.9 | 1.0 (1.0–1.1) | 0.8 | 0.4 (.4–.5) | 3.1 | 1.7 (1.5–2.0) | 1.8 |
Abbreviations: AI/AN, American Indian or Alaska Native; CI, confidence interval; IRR, incidence rate ratio; PI, Pacific Islander; Ref, reference category for IRR calculation.
aIncidence given as cases per 100 000 persons per year.
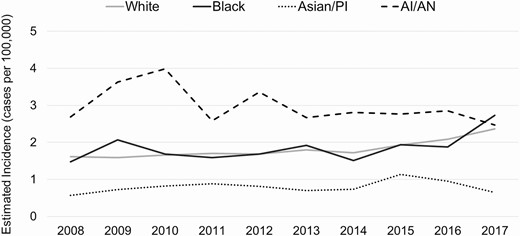
Trends in estimated annual incidence of invasive Haemophilus influenzae disease, by race (United States, 2008–2017). Abbreviations: AI/AN, American Indian or Alaska Native; PI, Pacific Islander.
Age trends for each racial group followed a similar pattern, with the highest average annual incidences observed among children aged <1 year and adults aged ≥65 years (Table 2). Incidence among children aged <1 year was highest among AI/AN children (34.9 cases/100 000), 4.4 times (95% CI, 3.1–6.2) the incidence for White children. Among adults aged ≥65 years, the incidence was also highest among AI/AN (9.4 cases/100 000), though not significantly higher than that among White older adults (IRR, 1.4 [95% CI, 1.0–2.0]). In every age group, Asian/PI persons had the lowest incidence.
By serotype, trends for White, Black, and Asian/PI populations were similar, with the highest incidence of disease due to NTHi, followed by Hif, then Hia and Hie, and finally Hib (Figure 2 and Supplementary Table 1). NTHi incidence increased notably among White and Black populations, with average annual increases of 4.4% (95% CI, 4.0%–4.8%) and 4.6% (3.7%–5.6%), respectively.
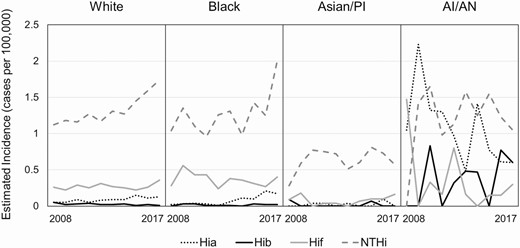
Trends in estimated annual incidence of invasive Haemophilus influenzae disease, by race and serotype (United States, 2008–2017). Note that the incidences of invasive H. influenzae serotypes c, d, and e are omitted here because they were low (<0.2 cases/100 000) among all races. Abbreviations: AI/AN, American Indian or Alaska Native; Hia, H. influenzae serotype a; Hib, H. influenzae serotype b; Hif, H. influenzae serotype f; NTHi, nontypeable H. influenzae; PI, Pacific Islander.
Serotype-specific incidence among AI/AN populations followed a different pattern than for all other races, though annual incidence was unsteady throughout the analysis period owing to small case counts and population sizes (Figure 2). Among AI/AN populations, NTHi and Hia contributed the highest burden, with incidences of 1.4 cases/100 000 and 1.0 cases/100 000, respectively (Supplementary Table 1). Hib incidence in AI/AN populations (0.4 cases/100 000) was substantially higher than in White, Black, and Asian/PI populations, which remained <0.1 cases/100 000.
Racial Disparities Among Children Aged <5 Years
From 2008 to 2017, a total of 823 cases of invasive H. influenzae disease among children aged <5 years were reported from ABCs sites. Of 766 cases with serotyped isolates (93.1%), 56.5% were NTHi, 21.7% Hia, 5.2% Hib, 2.2% Hie, and 14.4% Hif. By race, AI/AN children had the highest incidence of H. influenzae disease (13.8 cases/100 000), 5.3 times (95% CI: 4.2–6.8) the incidence among White children (2.6 cases/100 000; Table 3). Black children experienced an incidence of 4.1 cases/100 000, 1.6 times (95% CI, 1.4–1.9) higher than White children.
Estimated Average Annual Incidence of Invasive Haemophilus influenzae Disease Among Children Aged <5 Years, by Serotype and Race—United States, 2008–2017
| White | Black | Asian/PI | AI/AN | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Serotypea | Incidenceb | IRR | Incidenceb | IRR (95% CI) | Incidenceb | IRR (95% CI) | Incidenceb | IRR (95% CI) | Total Incidenceb |
| NTHi | 1.6 | Ref | 2.4 | 1.5 (1.2–1.9) | 1.4 | 0.9 (.6–1.4) | 2.0 | 1.2 (.7–2.3) | 1.7 |
| Hia | 0.5 | Ref | 0.6 | 1.3 (.9–1.9) | 0.1 | 0.1 (.0–.8) | 8.4 | 16.7 (11.7–24.0) | 0.7 |
| Hib | 0.1 | Ref | 0.1 | 0.4 (.1–1.3) | 0.0 | N/A | 2.9 | 22.4 (11.9–42.1) | 0.2 |
| Hie | 0.1 | Ref | 0.1 | 2.8 (1.0–7.1) | 0.1 | 1.2 (.1–8.9) | 0.0 | N/A | 0.1 |
| Hif | 0.3 | Ref | 0.9 | 2.8 (1.9–4.2) | 0.5 | 1.7 (.9–3.5) | 0.6 | 1.9 (.6–5.7) | 0.4 |
| Total | 2.6 | Ref | 4.1 | 1.6 (1.4–1.9) | 2.0 | 0.8 (.6–1.1) | 13.8 | 5.3 (4.2–6.8) | 3.0 |
| White | Black | Asian/PI | AI/AN | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Serotypea | Incidenceb | IRR | Incidenceb | IRR (95% CI) | Incidenceb | IRR (95% CI) | Incidenceb | IRR (95% CI) | Total Incidenceb |
| NTHi | 1.6 | Ref | 2.4 | 1.5 (1.2–1.9) | 1.4 | 0.9 (.6–1.4) | 2.0 | 1.2 (.7–2.3) | 1.7 |
| Hia | 0.5 | Ref | 0.6 | 1.3 (.9–1.9) | 0.1 | 0.1 (.0–.8) | 8.4 | 16.7 (11.7–24.0) | 0.7 |
| Hib | 0.1 | Ref | 0.1 | 0.4 (.1–1.3) | 0.0 | N/A | 2.9 | 22.4 (11.9–42.1) | 0.2 |
| Hie | 0.1 | Ref | 0.1 | 2.8 (1.0–7.1) | 0.1 | 1.2 (.1–8.9) | 0.0 | N/A | 0.1 |
| Hif | 0.3 | Ref | 0.9 | 2.8 (1.9–4.2) | 0.5 | 1.7 (.9–3.5) | 0.6 | 1.9 (.6–5.7) | 0.4 |
| Total | 2.6 | Ref | 4.1 | 1.6 (1.4–1.9) | 2.0 | 0.8 (.6–1.1) | 13.8 | 5.3 (4.2–6.8) | 3.0 |
Abbreviations: AI/AN, American Indian or Alaska Native; CI, confidence interval; Hia, Haemophilus influenzae serotype a; Hib, H. influenzae serotype b; Hie, H. influenzae serotype e; Hif, H. influenzae serotype f; IRR, incidence rate ratio; NTHi, nontypeable H. influenzae; PI, Pacific Islander; Ref, reference category for IRR calculation.
aNo cases of invasive disease due to H. influenzae serotype c or d were reported among children aged <5 years.
bIncidence given as cases per 100 000 persons per year.
Estimated Average Annual Incidence of Invasive Haemophilus influenzae Disease Among Children Aged <5 Years, by Serotype and Race—United States, 2008–2017
| White | Black | Asian/PI | AI/AN | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Serotypea | Incidenceb | IRR | Incidenceb | IRR (95% CI) | Incidenceb | IRR (95% CI) | Incidenceb | IRR (95% CI) | Total Incidenceb |
| NTHi | 1.6 | Ref | 2.4 | 1.5 (1.2–1.9) | 1.4 | 0.9 (.6–1.4) | 2.0 | 1.2 (.7–2.3) | 1.7 |
| Hia | 0.5 | Ref | 0.6 | 1.3 (.9–1.9) | 0.1 | 0.1 (.0–.8) | 8.4 | 16.7 (11.7–24.0) | 0.7 |
| Hib | 0.1 | Ref | 0.1 | 0.4 (.1–1.3) | 0.0 | N/A | 2.9 | 22.4 (11.9–42.1) | 0.2 |
| Hie | 0.1 | Ref | 0.1 | 2.8 (1.0–7.1) | 0.1 | 1.2 (.1–8.9) | 0.0 | N/A | 0.1 |
| Hif | 0.3 | Ref | 0.9 | 2.8 (1.9–4.2) | 0.5 | 1.7 (.9–3.5) | 0.6 | 1.9 (.6–5.7) | 0.4 |
| Total | 2.6 | Ref | 4.1 | 1.6 (1.4–1.9) | 2.0 | 0.8 (.6–1.1) | 13.8 | 5.3 (4.2–6.8) | 3.0 |
| White | Black | Asian/PI | AI/AN | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Serotypea | Incidenceb | IRR | Incidenceb | IRR (95% CI) | Incidenceb | IRR (95% CI) | Incidenceb | IRR (95% CI) | Total Incidenceb |
| NTHi | 1.6 | Ref | 2.4 | 1.5 (1.2–1.9) | 1.4 | 0.9 (.6–1.4) | 2.0 | 1.2 (.7–2.3) | 1.7 |
| Hia | 0.5 | Ref | 0.6 | 1.3 (.9–1.9) | 0.1 | 0.1 (.0–.8) | 8.4 | 16.7 (11.7–24.0) | 0.7 |
| Hib | 0.1 | Ref | 0.1 | 0.4 (.1–1.3) | 0.0 | N/A | 2.9 | 22.4 (11.9–42.1) | 0.2 |
| Hie | 0.1 | Ref | 0.1 | 2.8 (1.0–7.1) | 0.1 | 1.2 (.1–8.9) | 0.0 | N/A | 0.1 |
| Hif | 0.3 | Ref | 0.9 | 2.8 (1.9–4.2) | 0.5 | 1.7 (.9–3.5) | 0.6 | 1.9 (.6–5.7) | 0.4 |
| Total | 2.6 | Ref | 4.1 | 1.6 (1.4–1.9) | 2.0 | 0.8 (.6–1.1) | 13.8 | 5.3 (4.2–6.8) | 3.0 |
Abbreviations: AI/AN, American Indian or Alaska Native; CI, confidence interval; Hia, Haemophilus influenzae serotype a; Hib, H. influenzae serotype b; Hie, H. influenzae serotype e; Hif, H. influenzae serotype f; IRR, incidence rate ratio; NTHi, nontypeable H. influenzae; PI, Pacific Islander; Ref, reference category for IRR calculation.
aNo cases of invasive disease due to H. influenzae serotype c or d were reported among children aged <5 years.
bIncidence given as cases per 100 000 persons per year.
By serotype, NTHi accounted for the highest incidence of H. influenzae disease among children aged <5 years (1.7 cases/100 000; Table 3). NTHi incidence was highest among Black children (2.4 cases/100 000), 1.5 times (95% CI, 1.2–1.9) the incidence among White children. The largest disparity between Black and White children was in Hif disease (IRR, 2.8 [95% CI, 1.9–4.2]).
Hib and Hia were the primary causes of invasive H. influenzae disease among AI/AN children aged <5 years. Hib incidence was highest among AI/AN children (2.9 cases/100 000), 22.4 times higher than in White children (95% CI, 11.9–42.1; Table 3). Hia incidence was highest among AI/AN children (8.4 cases/100 000), 16.7 times higher than in White children (95% CI, 11.7–24.0). However, the incidence of Hia in AI/AN children declined by 11.7% annually (95% CI, −15.2% to −8.1%) during this period. Although the Hia incidence was relatively low (<1 cases/100 000) among White and Black children, recent increases were observed: a 13.6% annual increase (95% CI, 10.7%–16.5%) among White children and a 40.4% annual increase (32.1%–49.2%) among Black children (Figure 3 and Supplementary Figure 1).

Trends in estimated annual incidence of invasive Haemophilus influenzae serotype a disease among children aged <5 years, by race (United States, 2008–2017). Note that Supplementary Figure 1 includes a more detailed view of trends in estimated annual incidence of invasive H. influenzae serotype a disease among White and Black children aged <5 years. Abbreviations: AI/AN, American Indian or Alaska Native; PI, Pacific Islander.
We examined the Hib vaccination status of Hib cases reported to ABCs in children aged <5 years. Among 40 cases, 40% were in age-appropriately or fully vaccinated children. By race, 53.3% of Hib cases among AI/AN children were age appropriately or fully vaccinated, compared with 32.0% among White and Black children (P = .20; Supplementary Figure 2). Of age-appropriately and fully vaccinated children with Hib (all races), 44% received PRP-OMP, 31% received PRP-T, and 13% received PRP-CRM (Supplementary Table 2). Of age-appropriately or fully vaccinated AI/AN children with Hib, 75% received PRP-OMP.
Incidence Trends Among Adults Aged ≥65 Years
From 2008 to 2017, 45.4% of all invasive H. influenzae disease cases reported from ABCs sites (3352 of 7379) occurred in adults aged ≥65 years. After children aged <1 year, adults aged ≥65 years had the second highest incidence of invasive H. influenzae disease (6.6 cases/100 000; Table 2). Within each racial group, NTHi caused the highest incidence in this oldest age group (range, 3.2–5.7 cases/100 000; Supplementary Table 3). The NTHi incidence in adults aged ≥65 years increased among White and Black populations, with average annual increases of 2.9% (95% CI, 2.4%–3.4%) and 3.4% (1.7%–5.1%), respectively, though no pronounced racial disparities were identified. Hia and Hib incidences were significantly higher among AI/AN adults aged ≥65 years when compared with White populations (Hia IRR, 9.3 [95% CI, 3.5–21.8]; Hib IRR, 14.2 [4.6–52.0]).
DISCUSSION
In the Hib vaccine era, racial disparities in invasive H. influenzae disease persist. In the ABCs population, disparities affecting AI/AN populations were most evident, with the greatest disparity among AI/AN children aged <5 years who experienced elevated Hia and Hib incidence. White and Black populations showed similar disease trends, with incidence increasing in recent years, especially for Hia and NTHi. Asian/PI populations consistently had the lowest burden of invasive H. influenzae disease.
NTHi was the most common type of invasive H. influenzae disease within all racial groups. Though observed disparities in NTHi incidence were limited, Black children aged <5 years experienced an incidence of NTHi 1.5 times that of White children. A vaccine targeting NTHi could have substantial impact on invasive disease in all racial groups. Recently, a candidate NTHi vaccine (GSK2838504A) finished phase 2 clinical trials in adults at risk for acute exacerbations of chronic obstructive pulmonary disease [24]. While the candidate vaccine demonstrated an acceptable safety profile and was immunogenic, whether it can reduce NTHi carriage and prevent invasive disease remains to be determined.
Pronounced racial disparities in invasive Hia disease were identified. Consistent with other reports of increased Hia incidence among AI/AN communities [25–29], AI/AN children aged <5 years had the largest burden of Hia disease, nearly 17 times the incidence among White children. The Hia incidence was lower but rising 13.6% annually among White children and 40.4% annually among Black children. These results, combined with the similarities in clinical presentation and severity between Hia and Hib [30], indicate a growing need for prevention tools. In Canada, a similarly high incidence of Hia disease among indigenous populations prompted the National Research Council of Canada and the Public Health Agency of Canada to develop a Hia vaccine [31, 32], though clinical trials are awaiting funding [33].
In the pre-Hib vaccine era, invasive Hib incidence in Black and AI/AN children aged <5 years was estimated to be 3–4 times and 5–10 times higher, respectively, than in White children. Hib incidence estimates ranged from 24 to 66 cases/100 000 among White [5, 9], 104 to 219 cases/100 000 among Black [5, 9] and 214 to 705 cases/100 000 among AI/AN children [34, 35]. In the Hib vaccine era, invasive Hib incidence in children aged <5 years declined dramatically (>99%) among all races. Our analysis demonstrates that in the Hib vaccine era, racial disparities in invasive Hib disease have been eliminated among Black children but not among AI/AN children. According to these ABCs estimates, Hib incidence in AI/AN children remains 2.9 cases/100 000, more than 22 times that of White children and more than 10 times the Healthy People 2020 goal of 0.27 cases/100 000 [36]. The persistence of Hib disease among AI/AN children in the Hib vaccine era may reflect ongoing high nasopharyngeal colonization and transmission.
To address remaining Hib disease and disparities, evaluation of the current vaccination strategy is needed. Data from National Immunization Surveys indicate that coverage with the full Hib vaccine series in children aged 19–35 months is not significantly different among racial groups, though no racial group has met the Healthy People 2020 goal of 90% coverage [36]. In our analysis, most White and Black children with Hib were unvaccinated or undervaccinated, highlighting the need to increase vaccine uptake. More than half of AI/AN children with Hib were age appropriately vaccinated, primarily with PRP-OMP, suggesting susceptibility to Hib disease despite vaccination.
The Advisory Committee on Immunization Practices recommends that AI/AN children preferentially receive a Hib vaccine primary series containing PRP-OMP [19]. While PRP-OMP elicits protective antibodies after the first dose, the overall immunogenicity of the PRP-OMP series is lower than that of the PRP-T series [37]. Further evaluations are needed to determine the duration of protection in AI/AN children receiving the PRP-OMP vaccine series, and to determine whether there is a way to improve protection against invasive Hib disease.
To address racial disparities in invasive H. influenzae disease, updated evaluations of risk factors explaining these disparities are needed. Continued high rates of household crowding [38], poverty [39], and limited access to running water [40, 41] may be contributing factors to the elevated burden of disease among AI/AN populations. Inversely, the observed low incidence of invasive H. influenzae disease among Asian/PI populations may be partially due to lower reported rates of poverty [42].
This analysis had several limitations. First, race data were abstracted from medical charts rather than patient interview; for 9.1% of cases where race was missing, race was multiply imputed. Second, it is difficult to draw clear conclusions about disease trends among racial minorities owing to small case counts and unsteady incidence. Finally, though ABCs includes a similar proportion of AI/AN persons (1.5% in 2017) as in the general US population (1.4% in 2017) [18], the incidence of invasive H. influenzae is not uniform in all AI/AN communities. Notably, the reported Hia incidence in AI/AN children aged <5 years in Alaska (27.7 cases/100 000) [29] is >3 times that estimated by ABCs (8.4 cases/100 000). However, similar estimates of Hib incidence were noted in Alaska (2.8 cases/100 000) [26] and ABCs (2.9 cases/100 000). Despite these limitations, ABCs offers the ability to make national incidence projections, highlighting disparities in invasive H. influenzae disease for further investigation.
Our results indicate that racial disparities in invasive H. influenzae disease persist in the United States in the Hib vaccine era, despite remarkable reductions in Hib disease overall. AI/AN communities continue to experience disproportionately high rates of Hib disease. In addition, Hia disease disproportionately affects AI/AN communities, though Hia incidence among White and Black communities has recently increased. Evaluation of current Hib prevention strategies, efforts to increase Hib vaccine uptake, and new prevention tools for Hia and NTHi could help reduce the invasive H. influenzae disease burden overall and address remaining disparities.
Supplementary Data
Supplementary materials are available at Clinical Infectious Diseases online. Consisting of data provided by the authors to benefit the reader, the posted materials are not copyedited and are the sole responsibility of the authors, so questions or comments should be addressed to the corresponding author.
Notes
Acknowledgments. The authors are grateful to the following individuals for their contributions to the establishment and maintenance of the Active Bacterial Core surveillance system. California Emerging Infections Program: Susan Brooks and Hallie Randel. Colorado Emerging Infections Program: Benjamin White, Deborah Aragon, Meghan Barnes, and Jennifer Sadlowski. Connecticut Department of Public Health: Matt Cartter, Carmen Marquez, and Michelle Wilson. Georgia Emerging Infections Program: Stephanie Thomas, Amy Tunali, Wendy Baughman, Ashley Moore, Lauren Lorentzson, and Melissa Tobin-D’Angelo. Maryland Emerging Infections Program: Joanne Benton, Terresa Carter, Rosemary Hollick, Kim Holmes, and Kathleen Shutt. Minnesota Emerging Infections Program: Kathryn Como-Sabetti, Corinne Holtzman, Richard Danila, and Kerry MacInnes. New Mexico Emerging Infections Program: Kathy Angeles, Joseph Bareta, Lisa Butler, Nicole Espinoza, Sarah Khanlian, Robert Mansmann, Megin Nichols, and Lisa Onischuk. New York Emerging Infections Program: Suzanne McGuire, Alison Muse, Glenda Smith, Nancy Spina, and Rachel Wester. Oregon Emerging Infections Program: Mark Schmidt, Jamie Thompson, and Tasha Poissant. Tennessee Emerging Infections Program: Brenda Barnes, Karen Leib, Katie Dyer, Tiffanie Markus, and Lura McKnight. Arctic Investigations Program, Centers for Disease Control and Prevention (CDC): Debby Hurlburt, Danielle Lecy, Gail Thompson, Sara Seeman, Alisa Reasonover, and Carolynn Debyle. Division of Bacterial Diseases, CDC: Melissa Arvay, Olivia Almendares, and Huong Pham (Bacterial Meningitis Laboratory).
Disclaimer. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the CDC.
Financial support. This work was supported by a cooperative agreement with the Emerging Infections Program of the CDC (grant CDC-RFA-CK12-120205CONT16).
Potential conflicts of interest. L. H. H. has served as a consultant to GlaxoSmithKline, Merck, Pfizer, and Sanofi Pasteur. W. S. has served as a consultant to Merck, Pfizer, and Roche Diagnostics. All other authors report no potential conflicts.
All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.


{kind=link}
{kind=link}
{kind=link}