





Abstract
The inverted-V deformity is an unwanted aesthetic consequence of dorsal hump resection. Despite their attachment to the nasal bones, the upper lateral cartilages (ULCs) can separate from the nasal bones, creating a step-off after cartilaginous dorsal hump removal.
The mechanism of how the ULCs can separate from the nasal bones despite their attachment was studied to improve understanding of the inverted-V complication and its prevention.
A dorsal hump resection (bony and cartilaginous) was performed on 12 fresh cadavers to observe the effect on the ULCs. As a secondary study, the effect of different preventative maneuvers was investigated.
Cartilaginous dorsal resection destroys the spreader mechanism of the T-frame and impacts the stabilization of the ULCs, resulting in them becoming free-floating. This causes them to migrate in a posterior, medial, and cranial direction relative to the nasal bones. The dynamic attachment of the ULCs to the nasal bones is key in this mechanism and allows actual separation of the ULCs from the nasal bones to result in the inverted-V deformity. Caudal traction to the ULCs re-tensions these attachments, pulling the ULCs against the nasal bones again.
This anatomic dissection study has established that the connection between the nasal dorsum and ULCs is not a static fusion but is dynamic. This attachment can be used in primary rhinoplasty to prevent inverted-V deformity by applying caudal traction to the ULCs when reconstructing the dorsum which will tension the ULCs toward the nasal bones.
The inverted-V deformity is a complication that tends to occur as a sequel to dorsal hump resection.1 In this deformity, depression of the cephalic end of the upper lateral cartilages (ULCs) results in a step-off that allows the caudal edge of the nasal bones to become visible through the thin skin at the keystone area.
This cartilaginous collapse is ascribed to the loss of the spreader effect of the septal T-frame, allowing the ULCs to medialize. However, Straatsma demonstrated that the perichondrium of the ULCs and the periosteum of the nasal bones were fused at their side-to-side apposition.2 If this were true, the ULCs should remain attached to the nasal bones, maintaining a smooth transition without a step-off despite the loss of the spreading mechanism.
Roostaeian et al previously observed a natural tendency of the ULCs to recoil into a non-anatomical position after separation of the ULCs from the septum.3 A recent anatomic study on the keystone area did not demonstrate how the ULCs can medialize despite their attachment to the nasal bones.4 The principal goal of this study was to demonstrate the pathophysiology of this phenomenon.
METHODS
Ethical approval for the project was granted by the Human Ethics Advisory Group of the Queensland University of Technology (project number LR2021-4306-4761). The authors state that every effort was made to follow all local and international ethical guidelines and laws that pertain to the utilization of human cadaveric donors in anatomical research. The study was conducted from September to December 2021.
Twelve fresh non-embalmed cadavers were dissected, and the effect of a dorsal hump resection on the ULCs was assessed. The skin, subcutis, superficial musculoaponeurotic system, perichondrium, and periosteum were first removed from the nasal dorsum while preserving the perichondrium and periosteum in the keystone area to maintain the integrity of the connections between the nasal bones and the ULCs. The bony dorsum was then removed with an osteotome, leaving the cartilage intact. Finally, the cartilaginous dorsum was sharply incised and resected. In 3 cases, an extramucosal dissection was conducted, and in 9 cases the mucosa was removed with the hump resection. The resulting effect on the ULCs was noted.
Finally, the effect of external pressure on the ULCs was assessed in 4 different scenarios: (1) before dorsal hump resection, (2) after dorsal hump resection without preventative maneuvers, (3) after dorsal hump resection and insertion with spreader grafts of different thicknesses, and (4) after dorsal hump resection and the use of caudal traction. These effects were assessed in a qualitative (yes/no) rather than quantitative fashion because the subtlety of the collapse (max. = 2 mm) makes quantitative assessment subject to a significant error of measurement and observer bias and hence is unreliable.
RESULTS
On close inspection, the attachment between the ULCs and the nasal bones are revealed to be lengthy (1-2 mm), allowing some mobility of the ULCs relative to the nasal bones. When the dorsum is intact, the T-frame pushes the ULCs anteriorly, laterally, and caudally toward the nasal bones, tensioning the attachments and creating a fused appearance and a virtually seamless transition from nasal bone to a tense, relatively flat ULC.
Removal of the bony dorsum alone does not result in any displacement of the ULCs. Subsequent resection of the cartilaginous dorsum, some of which is partially hidden beneath the bony vault, or simple division of the ULCs from the septum results in a complete loss of the spreading T-frame, causing the ULCs to be free-floating. Once the T-frame is disrupted, the stress is released and the ULCs move posteriorly, medially, and cephalad into a “relaxed” position as if releasing the tension on a spring. This results in the step-off and the inverted-V. This did not differ in the 3 cases with preserved mucosa.
External pressure on this unstable cartilaginous dorsum (eg, by the skin envelope) aggravates this step-off by pushing the ULCs further in the posterior, medial, and cephalad direction. In the case of flimsy cartilages unable to provide any resistance, the untensioned ULCs additionally fold inward just caudal to the edge of the nasal bones, aggravating the step-off.
Spreader grafts or flaps effectively restore the anterior or medial part of the keystone area regardless of the caudal traction if they are of appropriate thickness. However, the lateral walls of the ULCs, posterior and lateral to the graft or flap, can still collapse and cause a step-off (Figure 1). In contrast, caudal traction on the ULCs fully reverses the step-off along the entire keystone, with the ULCs returning toward the nasal bones as well as being tensioned straight (Figure 2; Video 1). This position must be maintained by closing the roof with a spreader graft or flap, re-creating the T-piece, or grafting the dorsum. Subsequent scar formation will cause the final stable situation if the caudal tension is maintained for a sufficient time for this to occur.
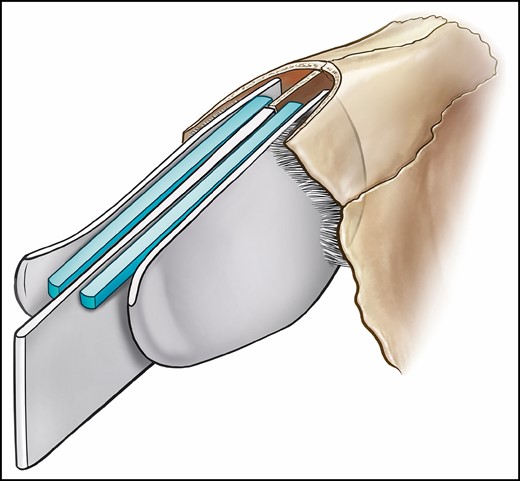
The isolated utilization of a spreader graft can be insufficient to push the upper lateral cartilages against the nasal bones. Even a graft of sufficient width to push the upper lateral cartilages against the nasal bones will not support the side walls, allowing collapse and a step-off across the lateral keystone.
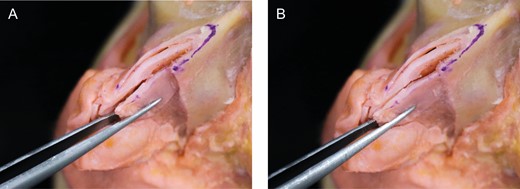
Anatomic dissection demonstrating the nose after dorsal hump resection, (A) before and (B) after caudal traction on the upper lateral cartilage. Note how this maneuver pulls the upper lateral cartilages back toward the nasal bone.
DISCUSSION
Pathophysiology of the Inverted-V Deformity
Traditional teaching suggests that an inverted-V deformity can be caused by 1 or a combination of the following 4 interventions: (1) over-resection of the cartilaginous dorsum, (2) avulsion of the ULCs from the nasal bones by accidentally slipping the periosteal elevator between ULC and nasal bone, (3) mucosal resection with scar retraction, or (4) loss of the spreader mechanism by removing the T-frame.1 The first intervention directly causes a step-off. The second intervention has never been demonstrated to cause an inverted-V by itself. Merely slipping the elevator under the nasal bone would not suffice to cause this but could potentially aggravate the situation in combination with any of the other causes. The third intervention can be prevented by performing an extramucosal dissection, avoiding subsequent mucosal scarring. However, the fourth intervention cannot be explained by conventional teaching because the fusion of the bone and the cartilage would supposedly prevent the ULCs from collapse, even if internal scarring or external pressure would pull/push the ULCs inward.
This study has revealed a tensioned attachment between the nasal bones and the ULCs. This attachment causes the ULCs to approximate the nasal bone when pushed or pulled caudally. This finding differs from the finding of Straatsma et al and Afrooz et al, who both suggested that the perichondrium of the ULCs and the periosteum of the nasal bones are fused at the area of apposition.2,4 We have found that the lengthy attachment allows some posterior, medial, and cephalad movement of the ULCs relative to the nasal bones. Like other prestressed tensegrity structures, this might have a protective function by increasing plasticity, preventing cartilage fracture in case of trauma. Regardless of its function, once the T-frame is disrupted and the ULCs are no longer pushed anteriorly, laterally, and caudally, the ULCs recoil posteriorly, medially, and cephalad, resulting in a step-off and the inverted-V deformity. The lack of tension in the ULCs allows further collapse, which explains why patients with short nasal bones and long ULCs are at higher risk for inverted-V deformity.5 The utilization of subperichondrial and subperiosteal dissection could potentially destabilize the keystone even further by destroying the splinting effect of this enveloping fascia. Similarly, the resting tension of the different nasal muscles might add to the stability, and the complex of muscles attached to the scroll ligaments may assist.6 It is therefore recommended to leave these attached if possible or reattach them if they are dissected off the scroll area.
Prevention of Inverted-V Deformity
Various modalities have been introduced in the prevention of the inverted-V deformity. Spreader grafts, introduced by Sheen in 1984, are regarded as the standard method for preventing collapse of the internal nasal valves and inverted-V deformity.1 In functional terms, the grafts move the ULCs away from the septum. Aesthetically, they widen the cartilaginous dorsum and push the ULCs toward the bony vault. Introduced by Oneal and Berkowitz in 1998, spreader flaps were proposed as an alternative without the need to harvest additional graft material.7 Infracture of the nasal bones can improve the width of the dorsum, reducing the necessary amount of spreading. However, these techniques may be insufficient to prevent an inverted-V deformity if insufficient width of the spreader graft/flap fails to push the superior part of the ULCs to the nasal bones.
This anatomic dissection study has confirmed that caudal traction on the ULCs brings them toward the nasal bones again, regardless of dorsal reconstruction maneuvers employed (Figure 3; Video 2). The tensioned lateral walls can also better withstand external forces. Finally, the caudal fixation of the ULCs might also help in the prevention of alar retraction by reducing cephalad migration of the lower lateral cartilages, which are attached to the ULCs at the scroll area. Therefore, we advocate maintaining caudal traction when reconstructing the dorsum utilizing any method.
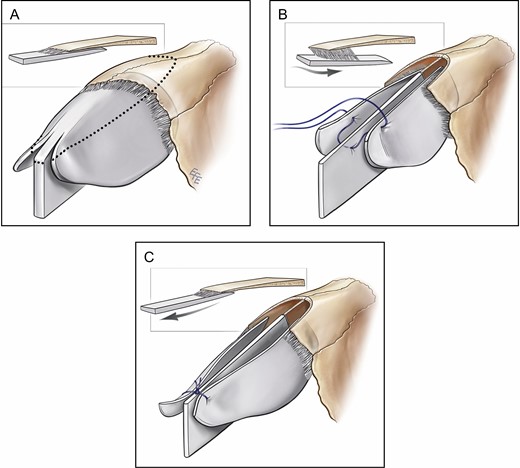
Illustration of the pathophysiology and the prevention of inverted-V deformity. (A) In an intact dorsum, the upper lateral cartilages are pushed anteriorly, laterally, and caudally against the nasal bones. (B) Dorsal hump resection causes the upper lateral cartilages to migrate posteriorly, medially, and cephalad, creating a step-off. (C) Caudal traction restores the anatomic relationship between the upper lateral cartilages and the nasal bones. Note that the suture is placed proximal to where the upper lateral cartilages diverge.
Various surgeons already believed that caudal traction on the ULCs adds to the structural stability of the rhinoplasty result. Rohrich et al previously described a technique of caudal traction, termed the “upper lateral cartilage tension spanning suture.” 3 However, the inverted-V still occurs, and this study might be what is required to transform belief into effective measures to prevent the deformity, especially because the prevention of inverted-V deformity by caudal traction in primary rhinoplasty is within the reach of all rhinoplasty surgeons.
A limitation to this anatomic cadaver study is that it did not factor in the effects of healing, contracture, and long-term changes to the construction. As with any suture, final stability relies on subsequent scarring after the procedure. The caudal tension-spanning suture presumably holds the ULCs in the right position for subsequent scarring to allow them to heal in the correct position, providing final stability. Important for this is the restoration of the roof, which allows the scarring to result in a stable structure. This can be accomplished by maneuvers such as the reconstitution of the dorsal T-piece, cartilage onlay graft, diced cartilage in fascia, spreader flaps, or spreader grafts. Another limitation is that the utilization of osteotomies was not studied, although there are no indications to suggest that osteotomies would change the relationship of the ULCs with the nasal bones unless the narrowed distance between nasal bones and septum allow the ULCs to impact the septum directly or indirectly such as with spreader grafts of flaps. The recent conversion of many hump reductions to let down or push down procedures in dorsal preservation rhinoplasty also preserves the septal T-frame and seems to eliminate the possibility of inverted-V, even with lateral keystone release (ballerina maneuver).8
Technical Nuances to Improve Outcomes
Understanding what happens after the cartilaginous dorsum is removed helps us understand how to reconstruct the inverted V deformity. We have been utilizing the caudal tension-spanning sutures for the last 8 years as an adjunct to dorsal reconstruction in structural rhinoplasty. A few remarks will help the efficacy of these sutures during surgery. The tension-spanning suture (5.0 PDS) is placed first before restoration of the roof and can be removed once the roof is restored in a manner that maintains the caudal traction, for example, by suturing spreader grafts or flaps under tension. However, when the roof is restored and stability is not maintained, such as with diced cartilage in fascia or replacement of the T piece, this suture should remain in place. When leaving the suture in place, it is important to not place the caudal tension-spanning suture at the very caudal end of the ULCs because the cartilages should be allowed to naturally diverge here; tension on each side must be appropriate to keep the septum straight.
The caudal tension-spanning suture only works in prevention of inverted-V deformity in a primary case, not in secondary correction of an inverted-V deformity. In the latter case, the virtual space between the ULCs and the nasal bone becomes scarred, and caudal pull will not approximate the ULCs toward the nasal bone.
CONCLUSIONS
This anatomic dissection study has confirmed that cartilaginous dorsum resection with removal of the T-frame results in recoil of the ULCs, potentially causing an inverted-V deformity. The key mechanism is the dynamic fibrous connection between the ULCs and nasal bones, previously understood to be an area of static fusion. Regardless of the method employed to restore the dorsum (spreader grafts, flaps, dorsal replacement), applying caudal traction when reattaching the ULCs in primary rhinoplasty initially restores the relationship between nasal bone and ULC. This will return the ULCs toward the nasal bones and restore the tension in the rest of the ULCs, preventing a step-off, ULC collapse, and inverted-V deformity.
Presented at: the Sydney Rhinoplasty Dissection Course (AAFPS) in Sydney, New South Wales, Australia in November 2021.
Disclosures
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors received no financial support for the research, authorship, and publication of this article.
REFERENCES
Author notes
Dr Callan is a specialist plastic surgeon in private practice in Geelong, Victoria, Australia


{kind=link}
{kind=link}
{kind=link}