





Abstract
Aspiration prior to hyaluronic acid filler injection is often taught as a safety maneuver to minimize the risk of intravascular injection; however, the validity of this technique in aesthetic practice is being increasingly challenged. One key assumption underpinning the validity of the aspiration test is that the needle tip does not move during the aspiration and subsequent injection of filler.
The aim of this study was to visualize and measure needle tip movement in real time during aspiration and injection of filler. Secondary objectives were to assess the impact of injector experience and double-handed versus single-handed aspiration technique in maintaining stability of the syringe.
Under real-time ultrasound visualization, 3 injectors with different levels of experience injected hyaluronic acid filler into pork belly tissue utilizing both double-handed and single-handed aspiration techniques. Needle tip movements were recorded and measured by means of ultrasound and video.
The aspiration maneuver is in all cases associated with retrograde movement of the needle tip, ranging from 1.1 to 5.3 mm (mean, 2.9 mm), whereas injection leads to anterograde movement ranging from 0.6 to 4.1 mm (mean, 1.9 mm). Double-handed aspiration is associated with less needle tip movement than single-handed aspiration (P = 0.037). Greater experience is also associated less movement of the needle tip (P < 0.0001).
In all cases, the aspiration and injecting maneuver is associated with micromovements of the needle tip, of a magnitude consistently significant relative to the typical size of facial vessels. Although needle tip movement is only a single factor limiting the usefulness of the aspiration test, the results of this study suggest that it is not advisable to rely only on aspiration as a method to prevent intravascular injection.
Resumen
La aspiración antes de la inyección de relleno de ácido hialurónico a menudo se enseña como una maniobra de seguridad para minimizar el riesgo de una inyección intravascular; sin embargo, cada vez se cuestiona más la validez de esta técnica en la práctica estética. Una suposición clave que sustenta la validez de la prueba de aspiración es que la punta de la aguja no se mueve durante la aspiración y la posterior inyección de relleno.
El objetivo de este estudio fue visualizar y medir el movimiento de la punta de la aguja en tiempo real durante la aspiración y durante la inyección de relleno. Los objetivos secundarios fueron evaluar el impacto de la experiencia del inyector y la técnica de aspiración a doble mano versus una sola mano en el mantenimiento de la estabilidad de la jeringa.
Bajo visualización de ultrasonido en tiempo real, 3 inyectores con diferentes niveles de experiencia inyectaron relleno de ácido hialurónico en tejido de vientre de cerdo utilizando técnicas de aspiración con doble mano y con una sola mano. Los movimientos de la punta de la aguja se registraron y midieron por medio de ultrasonido y video.
La maniobra de aspiración se asocia en todos los casos con un movimiento retrógrado de la punta de la aguja, que oscila entre 1.1 y 5.3 mm (2.9 mm de media), mientras que la inyección conduce a un movimiento anterógrado que oscila entre 0.6 y 4.1 mm (1.9 mm de media). La aspiración a doble mano se asocia con menos movimiento de la punta de la aguja que la aspiración con una sola mano (P = 0.037). Una mayor experiencia también está asociada a un menor movimiento de la punta de la aguja (P < 0.0001).
En todos los casos, la maniobra de aspiración e inyección se asocia a micromovimientos de la punta de la aguja, de una magnitud consistentemente significativa en relación con el tamaño típico de los vasos faciales. Aunque el movimiento de la punta de la aguja es solo un factor que limita la utilidad de la prueba de aspiración, los resultados de este estudio sugieren que no es aconsejable confiar solo en la aspiración como método para prevenir la inyección intravascular.
See the Commentary on this article .
Aspiration prior to hyaluronic acid filler injection is often taught as a safety measure to ensure that the needle tip has not inadvertently entered a blood vessel. Although anecdotally the practice is common in many areas of medicine, such as in anesthesia, its validity in aesthetic practice relating to filler injection is increasingly being challenged.1-7
One of the key pillars underpinning the validity of aspiration is the premise that once the needle tip has been placed in the desired injection area, it cannot move again. In other words, for the result of the aspiration to be meaningful, it requires the injector to hold the needle tip completely still during the aspiration maneuver (pull phase) and the subsequent injection (push phase). Although this may seem a simplistic goal for the experienced injector, no study to date has examined in real time the micromovement of the tip of the needle during the aspiration and injection maneuver. This study examines the movement of the tip of the needle during the aspiration and injection of hyaluronic acid filler in a soft tissue maneuver under real-time ultrasound.
METHODS
The overall aspiration and injection maneuver is divided into 3 phases (Table 1). For the aspiration test result to be valid, once the needle tip has reached the desired position (completion of Phase 1), the needle tip must remain still for Phases 2 and 3. Any movement between or during these 2 phases would invalidate the test result because the needle tip may have moved into or out of a vessel without the injector becoming aware.
Three Phases of the Filler Injection Maneuver
| Injection phase | Associated movement |
|---|---|
| Phase 1 | Needle insertion and positioning to the desired location for injection |
| Phase 2 | Aspiration phase (single- or double-handed) |
| Phase 3 | Injection phase |
| Injection phase | Associated movement |
|---|---|
| Phase 1 | Needle insertion and positioning to the desired location for injection |
| Phase 2 | Aspiration phase (single- or double-handed) |
| Phase 3 | Injection phase |
Three Phases of the Filler Injection Maneuver
| Injection phase | Associated movement |
|---|---|
| Phase 1 | Needle insertion and positioning to the desired location for injection |
| Phase 2 | Aspiration phase (single- or double-handed) |
| Phase 3 | Injection phase |
| Injection phase | Associated movement |
|---|---|
| Phase 1 | Needle insertion and positioning to the desired location for injection |
| Phase 2 | Aspiration phase (single- or double-handed) |
| Phase 3 | Injection phase |
However, irrespective of whether a single- or a double-handed aspiration test is performed, the maneuver requires the injector to apply a “pull,” followed by a “push” force on the plunger. Necessarily, this requires a change in finger and often hand position to enable activation of different forearm muscle groups to apply these opposing forces on the plunger.
To precisely study the position of the needle during these maneuvers, 3 injectors were asked to inject hyaluronic acid filler into pork belly tissue. The movement of the needle tip was examined and recorded under real-time ultrasound during the 3 phases of the injection maneuver.
Three injectors with different levels of experience were recruited: a specialist plastic surgeon who is an experienced injector, a doctor in a surgical training position of intermediate experience level, and an operating theatre nurse who had no injection training. Each injector was instructed to inject in the 3 distinct phases while maintaining the needle tip as still as possible. Six attempts were recorded for each injector, 3 by single-handed aspiration (Figure 1) and 3 by a double-handed aspiration technique (Figure 2). Once the desired aspiration pressure was reached, the position had to be held for 3 seconds before 0.1 mL of filler was injected in Phase 3.
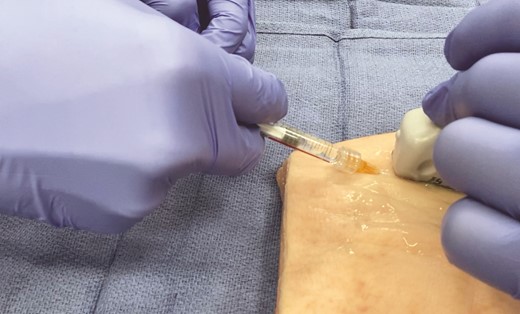
Single-handed aspiration test.

Double-handed aspiration test. The nondominant hand is used to stabilize the syringe while the dominant hand performs the aspiration test.
The needle tip position was recorded in the x and y planes during and at the end of each phase, and the overall maneuver was recorded both on ultrasound and video. Ultrasound examination was performed with a Fujifilm Sonosite X-Porte (Fujifilm Corporation, Tokyo, Japan) equipped with an HFL50xp, 15-6 MHz transducer optimized for breast and musculoskeletal tissue. Standard 1-mL syringes of Belotero Intense hyaluronic acid filler (Merz Australia Pty Ltd, Sydney, Australia) were used. Although most practitioners tend to perform injections with manufacturer-supplied 0.5-inch 27G to 30G needles, a 1-inch 25G needle was used for this study to allow for better visualization and for precise localization of the tip under ultrasound. Two 30-cm × 35-cm pieces of pork belly tissue, heated to room temperature, served as the target tissue. The study was approved at the Eastern Health Research Meeting and was conducted in accordance with the principles of the 1975 Declaration of Helsinki.
Statistical Analysis
Quantitative variables were described by their mean, standard deviation, and range. Movement, as indicated by changes in the needle tip position between each phase and between injectors, was compared and analyzed by paired t test. Differences were considered significant at P < 0.05. Statistical analysis was performed with Wizard Software Solutions (Chicago, IL) for MacOS v. 1.9.37 (Apple, Cupertino, CA).
RESULTS
Table 2 shows the results of the ultrasound measurement of needle tip movement through all 3 phases. Figure 3 shows an example of the injection maneuver visualized under ultrasound for Injector 1. (See Video available in the Supplemental Material.)
Results of Needle Tip Movement in the x and y Planes
| Phase 2 deviation (mm) | Phase 3 deviation (mm) | Final position deviation (mm) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| x | y | Deviation | x | y | Deviation | x | y | Deviation | ||
| Injector 1 | Double 1 | –1.9 | 1.0 | 2.1 | 0.6 | 0.9 | 1.1 | –1.1 | 0.6 | 1.3 |
| Double 2 | –1.1 | 0.1 | 1.1 | 0.7 | –0.7 | 1.0 | –0.5 | –0.9 | 1.0 | |
| Double 3 | –2.4 | 0.4 | 2.4 | 0.7 | –0.2 | 0.7 | –1.4 | –0.1 | 1.4 | |
| Double mean | 1.9 | 0.9 | 1.2 | |||||||
| Single 1 | –2.4 | 0.6 | 2.5 | –0.3 | 0.5 | 0.6 | –1.7 | 0.7 | 1.8 | |
| Single 2 | –2.1 | 0.9 | 2.3 | 0.8 | 0.4 | 0.9 | –0.4 | 0.4 | 0.6 | |
| Single 3 | –2.4 | 0.4 | 2.4 | 1.1 | –0.2 | 1.1 | –0.6 | 0.4 | 0.7 | |
| Single mean | 2.4 | 0.9 | 1.0 | |||||||
| Overall Mean | 2.1 | 0.9 | 1.1 | |||||||
| Injector 2 | Double 1 | –3.3 | 2.0 | 3.9 | –2.8 | 1.8 | 3.3 | –2.3 | 2.6 | 3.5 |
| Double 2 | –3.6 | 2.2 | 4.2 | –2.2 | 1.8 | 2.8 | –2.4 | 2.2 | 3.3 | |
| Double 3 | –3.5 | 2.2 | 4.1 | –2.6 | 2.0 | 3.3 | –1.8 | 1.9 | 2.6 | |
| Double mean | 4.1 | 3.2 | 3.1 | |||||||
| Single 1 | –4.3 | 1.8 | 4.7 | –3.2 | 1.1 | 3.4 | –1.7 | 1.4 | 2.2 | |
| Single 2 | –3.4 | 1.4 | 3.7 | –2.5 | 0.8 | 2.6 | 1.9 | –0.4 | 1.9 | |
| Single 3 | –5.2 | 1.2 | 5.3 | –4.0 | 1.0 | 4.1 | –1.4 | 1.8 | 2.3 | |
| Single mean | 4.6 | 3.4 | 2.1 | |||||||
| Overall Mean | 4.3 | 3.3 | 2.6 | |||||||
| Injector 3 | Double 1 | –2.0 | 1.6 | 2.6 | –1.8 | 1.4 | 2.3 | –1.2 | 1.0 | 1.6 |
| Double 2 | –1.9 | 0.7 | 2.0 | –1.2 | 1.2 | 1.7 | –0.8 | 0.8 | 1.1 | |
| Double 3 | –1.4 | 0.6 | 1.5 | –0.9 | 0.6 | 1.1 | –0.7 | –0.5 | 0.9 | |
| Double mean | 2.0 | 1.7 | 1.2 | |||||||
| Single 1 | –2.6 | 0.0 | 2.6 | –1.0 | –0.1 | 1.0 | 0.6 | 0.4 | 0.7 | |
| Single 2 | –2.3 | 0.7 | 2.4 | –1.4 | –0.5 | 1.5 | 0.8 | –0.4 | 0.9 | |
| Single 3 | –2.9 | 0.6 | 3.0 | –1.1 | –0.5 | 1.2 | 1.7 | –0.6 | 1.8 | |
| Single mean | 2.7 | 1.2 | 1.1 | |||||||
| Overall Mean | 2.3 | 1.5 | 1.2 |
| Phase 2 deviation (mm) | Phase 3 deviation (mm) | Final position deviation (mm) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| x | y | Deviation | x | y | Deviation | x | y | Deviation | ||
| Injector 1 | Double 1 | –1.9 | 1.0 | 2.1 | 0.6 | 0.9 | 1.1 | –1.1 | 0.6 | 1.3 |
| Double 2 | –1.1 | 0.1 | 1.1 | 0.7 | –0.7 | 1.0 | –0.5 | –0.9 | 1.0 | |
| Double 3 | –2.4 | 0.4 | 2.4 | 0.7 | –0.2 | 0.7 | –1.4 | –0.1 | 1.4 | |
| Double mean | 1.9 | 0.9 | 1.2 | |||||||
| Single 1 | –2.4 | 0.6 | 2.5 | –0.3 | 0.5 | 0.6 | –1.7 | 0.7 | 1.8 | |
| Single 2 | –2.1 | 0.9 | 2.3 | 0.8 | 0.4 | 0.9 | –0.4 | 0.4 | 0.6 | |
| Single 3 | –2.4 | 0.4 | 2.4 | 1.1 | –0.2 | 1.1 | –0.6 | 0.4 | 0.7 | |
| Single mean | 2.4 | 0.9 | 1.0 | |||||||
| Overall Mean | 2.1 | 0.9 | 1.1 | |||||||
| Injector 2 | Double 1 | –3.3 | 2.0 | 3.9 | –2.8 | 1.8 | 3.3 | –2.3 | 2.6 | 3.5 |
| Double 2 | –3.6 | 2.2 | 4.2 | –2.2 | 1.8 | 2.8 | –2.4 | 2.2 | 3.3 | |
| Double 3 | –3.5 | 2.2 | 4.1 | –2.6 | 2.0 | 3.3 | –1.8 | 1.9 | 2.6 | |
| Double mean | 4.1 | 3.2 | 3.1 | |||||||
| Single 1 | –4.3 | 1.8 | 4.7 | –3.2 | 1.1 | 3.4 | –1.7 | 1.4 | 2.2 | |
| Single 2 | –3.4 | 1.4 | 3.7 | –2.5 | 0.8 | 2.6 | 1.9 | –0.4 | 1.9 | |
| Single 3 | –5.2 | 1.2 | 5.3 | –4.0 | 1.0 | 4.1 | –1.4 | 1.8 | 2.3 | |
| Single mean | 4.6 | 3.4 | 2.1 | |||||||
| Overall Mean | 4.3 | 3.3 | 2.6 | |||||||
| Injector 3 | Double 1 | –2.0 | 1.6 | 2.6 | –1.8 | 1.4 | 2.3 | –1.2 | 1.0 | 1.6 |
| Double 2 | –1.9 | 0.7 | 2.0 | –1.2 | 1.2 | 1.7 | –0.8 | 0.8 | 1.1 | |
| Double 3 | –1.4 | 0.6 | 1.5 | –0.9 | 0.6 | 1.1 | –0.7 | –0.5 | 0.9 | |
| Double mean | 2.0 | 1.7 | 1.2 | |||||||
| Single 1 | –2.6 | 0.0 | 2.6 | –1.0 | –0.1 | 1.0 | 0.6 | 0.4 | 0.7 | |
| Single 2 | –2.3 | 0.7 | 2.4 | –1.4 | –0.5 | 1.5 | 0.8 | –0.4 | 0.9 | |
| Single 3 | –2.9 | 0.6 | 3.0 | –1.1 | –0.5 | 1.2 | 1.7 | –0.6 | 1.8 | |
| Single mean | 2.7 | 1.2 | 1.1 | |||||||
| Overall Mean | 2.3 | 1.5 | 1.2 |
“Phase 2 deviation” indicates the maximal change in position of the needle tip during aspiration (Phase 2) compared with the starting position (end of Phase 1). “Deviation” indicates the distance from starting position as calculated from Pythagoras’ theorem based on deviations in the x and y planes. “Phase 3 deviation” indicates the maximal change in position of the needle tip during the injection phase compared with the starting position (end of Phase 1). “Final position deviation” indicates the final position of the needle tip at the completion of Phase 3 compared with the starting position.
Results of Needle Tip Movement in the x and y Planes
| Phase 2 deviation (mm) | Phase 3 deviation (mm) | Final position deviation (mm) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| x | y | Deviation | x | y | Deviation | x | y | Deviation | ||
| Injector 1 | Double 1 | –1.9 | 1.0 | 2.1 | 0.6 | 0.9 | 1.1 | –1.1 | 0.6 | 1.3 |
| Double 2 | –1.1 | 0.1 | 1.1 | 0.7 | –0.7 | 1.0 | –0.5 | –0.9 | 1.0 | |
| Double 3 | –2.4 | 0.4 | 2.4 | 0.7 | –0.2 | 0.7 | –1.4 | –0.1 | 1.4 | |
| Double mean | 1.9 | 0.9 | 1.2 | |||||||
| Single 1 | –2.4 | 0.6 | 2.5 | –0.3 | 0.5 | 0.6 | –1.7 | 0.7 | 1.8 | |
| Single 2 | –2.1 | 0.9 | 2.3 | 0.8 | 0.4 | 0.9 | –0.4 | 0.4 | 0.6 | |
| Single 3 | –2.4 | 0.4 | 2.4 | 1.1 | –0.2 | 1.1 | –0.6 | 0.4 | 0.7 | |
| Single mean | 2.4 | 0.9 | 1.0 | |||||||
| Overall Mean | 2.1 | 0.9 | 1.1 | |||||||
| Injector 2 | Double 1 | –3.3 | 2.0 | 3.9 | –2.8 | 1.8 | 3.3 | –2.3 | 2.6 | 3.5 |
| Double 2 | –3.6 | 2.2 | 4.2 | –2.2 | 1.8 | 2.8 | –2.4 | 2.2 | 3.3 | |
| Double 3 | –3.5 | 2.2 | 4.1 | –2.6 | 2.0 | 3.3 | –1.8 | 1.9 | 2.6 | |
| Double mean | 4.1 | 3.2 | 3.1 | |||||||
| Single 1 | –4.3 | 1.8 | 4.7 | –3.2 | 1.1 | 3.4 | –1.7 | 1.4 | 2.2 | |
| Single 2 | –3.4 | 1.4 | 3.7 | –2.5 | 0.8 | 2.6 | 1.9 | –0.4 | 1.9 | |
| Single 3 | –5.2 | 1.2 | 5.3 | –4.0 | 1.0 | 4.1 | –1.4 | 1.8 | 2.3 | |
| Single mean | 4.6 | 3.4 | 2.1 | |||||||
| Overall Mean | 4.3 | 3.3 | 2.6 | |||||||
| Injector 3 | Double 1 | –2.0 | 1.6 | 2.6 | –1.8 | 1.4 | 2.3 | –1.2 | 1.0 | 1.6 |
| Double 2 | –1.9 | 0.7 | 2.0 | –1.2 | 1.2 | 1.7 | –0.8 | 0.8 | 1.1 | |
| Double 3 | –1.4 | 0.6 | 1.5 | –0.9 | 0.6 | 1.1 | –0.7 | –0.5 | 0.9 | |
| Double mean | 2.0 | 1.7 | 1.2 | |||||||
| Single 1 | –2.6 | 0.0 | 2.6 | –1.0 | –0.1 | 1.0 | 0.6 | 0.4 | 0.7 | |
| Single 2 | –2.3 | 0.7 | 2.4 | –1.4 | –0.5 | 1.5 | 0.8 | –0.4 | 0.9 | |
| Single 3 | –2.9 | 0.6 | 3.0 | –1.1 | –0.5 | 1.2 | 1.7 | –0.6 | 1.8 | |
| Single mean | 2.7 | 1.2 | 1.1 | |||||||
| Overall Mean | 2.3 | 1.5 | 1.2 |
| Phase 2 deviation (mm) | Phase 3 deviation (mm) | Final position deviation (mm) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| x | y | Deviation | x | y | Deviation | x | y | Deviation | ||
| Injector 1 | Double 1 | –1.9 | 1.0 | 2.1 | 0.6 | 0.9 | 1.1 | –1.1 | 0.6 | 1.3 |
| Double 2 | –1.1 | 0.1 | 1.1 | 0.7 | –0.7 | 1.0 | –0.5 | –0.9 | 1.0 | |
| Double 3 | –2.4 | 0.4 | 2.4 | 0.7 | –0.2 | 0.7 | –1.4 | –0.1 | 1.4 | |
| Double mean | 1.9 | 0.9 | 1.2 | |||||||
| Single 1 | –2.4 | 0.6 | 2.5 | –0.3 | 0.5 | 0.6 | –1.7 | 0.7 | 1.8 | |
| Single 2 | –2.1 | 0.9 | 2.3 | 0.8 | 0.4 | 0.9 | –0.4 | 0.4 | 0.6 | |
| Single 3 | –2.4 | 0.4 | 2.4 | 1.1 | –0.2 | 1.1 | –0.6 | 0.4 | 0.7 | |
| Single mean | 2.4 | 0.9 | 1.0 | |||||||
| Overall Mean | 2.1 | 0.9 | 1.1 | |||||||
| Injector 2 | Double 1 | –3.3 | 2.0 | 3.9 | –2.8 | 1.8 | 3.3 | –2.3 | 2.6 | 3.5 |
| Double 2 | –3.6 | 2.2 | 4.2 | –2.2 | 1.8 | 2.8 | –2.4 | 2.2 | 3.3 | |
| Double 3 | –3.5 | 2.2 | 4.1 | –2.6 | 2.0 | 3.3 | –1.8 | 1.9 | 2.6 | |
| Double mean | 4.1 | 3.2 | 3.1 | |||||||
| Single 1 | –4.3 | 1.8 | 4.7 | –3.2 | 1.1 | 3.4 | –1.7 | 1.4 | 2.2 | |
| Single 2 | –3.4 | 1.4 | 3.7 | –2.5 | 0.8 | 2.6 | 1.9 | –0.4 | 1.9 | |
| Single 3 | –5.2 | 1.2 | 5.3 | –4.0 | 1.0 | 4.1 | –1.4 | 1.8 | 2.3 | |
| Single mean | 4.6 | 3.4 | 2.1 | |||||||
| Overall Mean | 4.3 | 3.3 | 2.6 | |||||||
| Injector 3 | Double 1 | –2.0 | 1.6 | 2.6 | –1.8 | 1.4 | 2.3 | –1.2 | 1.0 | 1.6 |
| Double 2 | –1.9 | 0.7 | 2.0 | –1.2 | 1.2 | 1.7 | –0.8 | 0.8 | 1.1 | |
| Double 3 | –1.4 | 0.6 | 1.5 | –0.9 | 0.6 | 1.1 | –0.7 | –0.5 | 0.9 | |
| Double mean | 2.0 | 1.7 | 1.2 | |||||||
| Single 1 | –2.6 | 0.0 | 2.6 | –1.0 | –0.1 | 1.0 | 0.6 | 0.4 | 0.7 | |
| Single 2 | –2.3 | 0.7 | 2.4 | –1.4 | –0.5 | 1.5 | 0.8 | –0.4 | 0.9 | |
| Single 3 | –2.9 | 0.6 | 3.0 | –1.1 | –0.5 | 1.2 | 1.7 | –0.6 | 1.8 | |
| Single mean | 2.7 | 1.2 | 1.1 | |||||||
| Overall Mean | 2.3 | 1.5 | 1.2 |
“Phase 2 deviation” indicates the maximal change in position of the needle tip during aspiration (Phase 2) compared with the starting position (end of Phase 1). “Deviation” indicates the distance from starting position as calculated from Pythagoras’ theorem based on deviations in the x and y planes. “Phase 3 deviation” indicates the maximal change in position of the needle tip during the injection phase compared with the starting position (end of Phase 1). “Final position deviation” indicates the final position of the needle tip at the completion of Phase 3 compared with the starting position.

(A) Movement of the needle tip visualized by ultrasound during Phases 1 to 3. (B) Final needle tip position relative to starting position.
Aspiration Phase (Phase 2)
In all cases, aspiration was associated with retrograde movement of the needle tip along the trajectory of the body of the needle. This movement ranged from 1.1 to 5.3 mm, with mean values of 2.1 mm for Injector 1, 4.3 mm for Injector 2, and 2.3 mm for Injector 3 (Figure 4).
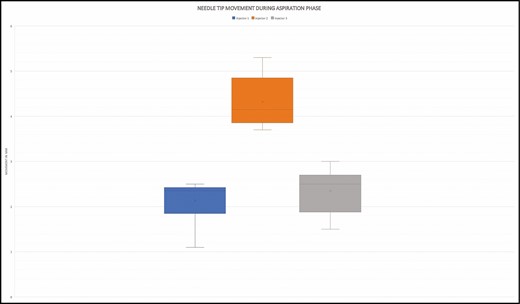
Needle tip movement during aspiration phase.
For all injectors, double-handed aspiration was associated with less needle tip movement, and hence greater stability during aspiration, than a single-handed technique (P = 0.037). When double-handed aspiration was performed there was a mean decrease in needle tip deviation vs single-handed aspiration of 0.5 mm for Injector 1, 0.5 mm for Injector 2, and 0.7 mm for Injector 3 (Figure 5).
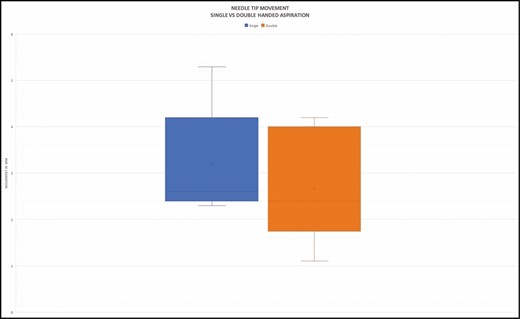
Single- vs double-handed aspiration.
Injection Phase (Phase 3)
In all cases, filler injection was associated with anterograde movement of the needle tip. This ranged from 0.6 to 4.1 mm of movement from the starting point of the needle at the end of Phase 1. The mean deviation was 0.9 mm for Injector 1, 3.3 mm for Injector 2, and 1.5 mm for Injector 3 (Figure 6).
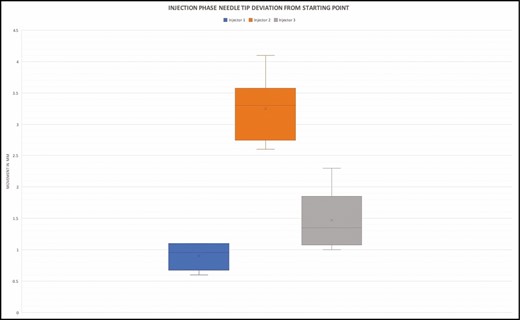
Injection-phase needle tip deviation.
Final Position of Needle Tip
In all cases, the final resting position of the needle tip deviated from the starting position. This deviation ranged from 0.6 to 3.5 mm, with mean values of 1.1 mm for Injector 1, 2.6 mm for Injector 2, and 1.2 mm for Injector 3 (Figure 7).
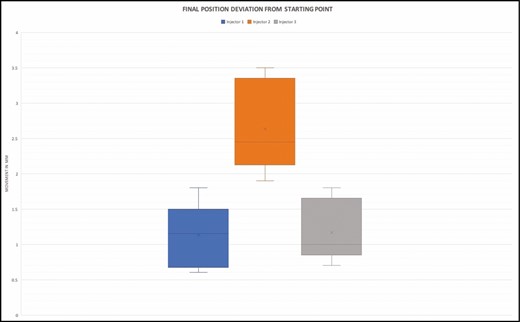
Final needle tip position deviation.
Impact of Experience
The 3 volunteer injectors were chosen based on their range of cosmetic injecting experience. Comparison of the needle tip movement during the aspiration phase showed a mean deviation of 2.1 mm for the most experienced injector (Injector 1), compared with 4.3 mm for the least experienced injector (Injector 2). Similarly, needle tip movement during the injection phase showed a mean deviation of 0.9 mm for Injector 1 compared with 3.3 mm for Injector 3. Overall, there was significantly less movement in the most experienced injector’s hands compared with the least experienced injector (P < 0.0001) (Figure 8).
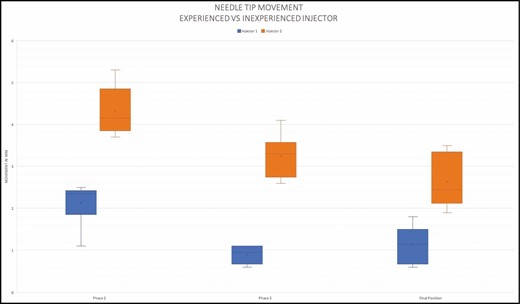
Impact of injector experience on needle tip movement..
Discussion
Aspiration before injecting is frequently taught to medical and nursing practitioners as an important safety measure to prevent inadvertent intravascular injections. In recent years, its validity has been questioned in many fields of general medical practice, including aesthetic medicine.1-3,8,9
Some of the concerns raised relate to the low specificity of the aspiration test, pertaining to its reliability when an apparent negative result is produced. In particular, questions have been raised about the use of needles vs cannulas for the aspiration,5,6,10,11 the needle/cannula gauge,5,12 the viscosity and elastic modulus (G′) of the filler product, variabilities in the pullback pressure, and the duration of aspiration.4,7,13
One of the critical tenets underpinning the validity of the aspiration test is the requirement that the needle tip must not move during the aspiration and the subsequent filler injection. Any movement, even of the order of millimeters, might mean the needle tip has moved into or out of a vessel. This is particularly relevant for filler injections of the face, where even named facial vessels have diameters of the order of 1 to 2 mm.14
The results of our ultrasound study demonstrate that movement of the needle tip occurs with each phase of the injection cycle in every attempt and for all injectors. As one would expect, retrograde motion is associated with aspiration and anterograde with injection, in keeping with the vector and the force applied to the plunger. This is relevant as significant pullback pressure (0.2-0.5 mL) and duration (3-10 seconds) is necessary to produce a valid aspiration test.5,7 In addition, micromovements occur between each phase as the aspiration maneuver changes to an injection maneuver. This transition necessitates changes in hand and finger position, as different flexor or extensor muscle groups are recruited to reverse the force applied to the plunger. In all cases, the double-handed aspiration test is shown to be more stable and associated with less movement than a single-handed technique.
Our study did not examine the effect of injecting on periosteum, which conceivably could limit the anterograde component of needle micromovement particularly during Phase 3. However, several authors have noted that in anatomic studies, injecting vertically on periosteum still results in product deposition in multiple anatomic planes, limiting the usefulness of this approach in reducing the risk of intravascular injection.15,16
The study is also limited by the fact that the injectors are performing in an ideal environment, seated comfortably with elbow supported, free from time pressure, distractions, or the need to deliver aesthetic results. It is also important to realize that a patient, often fraught with anxiety, would normally lie at the other end of the needle. Patient movement, even minute reactive or mimetic actions such as head turning, grimacing, flinching, speaking, or even drawing a deep breath, will shift entire tissue planes relative to the needle tip.
Conclusions
Although every effort to improve the safety of aesthetic injections should be applauded, the use of the aspiration test prior to injecting has consistently been challenged in previous publications. Our study has found that the injecting maneuver is associated with micromovements of the needle tip, which are consistently significant relative to the typical size of facial vessels. Although needle tip movement is just one factor limiting the usefulness of the aspiration test, the results of this study suggest that it is not advisable to rely only on the aspiration test as a method to prevent intravascular injection. Other safe practices, such as continuous needle movement and microbolus, may prove more reliable and we recommend that these should be considered as alternatives to aspiration.
Disclosures
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
Hyaluronic acid fillers were donated for the study by Merz Australia Pty Ltd (New South Wales, Australia).
References
Author notes
Dr Callan is a specialist plastic surgeon in private practice in Geelong, Victoria, Australia
Dr Roberts is an aesthetic physician in private practice in Melbourne, Victoria, Australia
Dr Hart is an aesthetic physician in private practice in Auckland, New Zealand
Dr Liew is a plastic surgeon in private practice in Darlinghurst, NSW, Australia
Dr Porter is an aesthetic practitioner in private practice in Darlinghurst, NSW, Australia
Dr Corduff is a specialist plastic surgeon in private practice in Geelong, Victoria, Australia
Mr Clague is an aesthetic injecting nurse in private practice in South Yarra, Victoria, Australia


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}