





Abstract
The aged and unattractive appearance of the neck has a profound impact on the overall youthfulness and attractiveness of the face. Neck wrinkles are one of the manifestations of neck skin aging. Botulinum toxin type A (BTX-A) represents an effective means for aesthetic neck rejuvenation as novel facial rejuvenation technologies are progressively developed.
The objective of this article was to review the pertinent clinical literature for descriptions of BTX-A treatments and evaluations of their efficacy and safety for neck wrinkles.
The Web of Science, PubMed, EMBASE, Cochrane Library, and SCOPUS databases were searched from inception to April 30, 2020, for the existing literature, which is presented along with the authors’ experience with neck wrinkles.
Overall, 112 women between 24 and 65 years of age were included in 3 studies of monotherapy and 2 studies of multimodal combination therapy. BTX-A has been reported in combination with other approaches, including intensity focused ultrasound, cohesive polydensified matrix hyaluronic acid, and microfocused ultrasound. Only 1 of the 3 reports on monotherapy had a less than 50% satisfaction and improvement rate. Overall, BTX-A attained high patient satisfaction without serious and persistent side effects, notwithstanding the relatively limited sample size.
The existing research cannot strongly prove the aesthetic effect of BTX-A in neck wrinkles. However, BTX-A is probably an effective technology in response to the growing demand for neck wrinkle treatment, whether in a single treatment or combined treatment.

Neck aging is frequently one of the first signs of multiple senescent changes. With an increasing trend of patients seeking a “younger” look, the aging of the neck has increasingly become an important problem for beauty seekers. This trend has spawned a dramatic increase in techniques and concepts for the treatment of the aging neck. The aesthetic deficiencies of the neck can be divided into contour changes (such as platysmal bands, rhytidosis and midneck hollowing, submental fat pads, or poorly defined jawlines) and skin aging changes (such as neck wrinkles, sagging skin, rough texture, and dark spots).1,2 Brandt et al3 published a paper in which they described 4 distinct categories of age-related neck degeneration. The skin on the neck is thinner, and there are fewer sebaceous glands. Due to the lack of moisture, the skin is prone to dryness, coupled with the loss of collagen and the atrophy of connective tissue; therefore, changes in the performance of the neck skin are more obvious and appear earlier than the contour change.4 Internal factors (such as race, genetic factors, oxidative stress hormones, and systemic diseases) and external factors (such as smoking, environmental factors, gravity, bad posture, and alcohol consumption) are all associated with neck aging.2,5 The factors affecting the formation of neck wrinkles are complex and diversified. The patients who ask for help with their neck lines tend to be younger, which is connected to the fact that these people frequently have the head-down posture related to work on mobile phones, computers, and so on. Therefore, neck wrinkles have been acknowledged as a key feature of age-related neck degeneration, and they are not exclusive to older people. With public awareness of neck aesthetics improving, researchers and clinical workers have begun to pay more attention to neck aesthetic changes.
Since botulinum toxin was approved by the US Food and Drug Administration for cosmetic treatment of glabella frown lines in April 2002, it is now extensively employed for cosmetic concerns. In clinical practice, botulinum toxin type A (BTX-A) products mainly include the United States type (onabotulinum toxin A [Botox]), the British type (abobotulinum toxin A [Dysport]), the German type (incobotulinum toxin A [Xeomin]), and the Chinese type (Hengli [Prosigne]). Different formulations of BTX-A have similar action principles, most of which involve actions on neuromuscular junctions through neurotoxin active molecules to inhibit the release of synaptic acetylcholine and promote muscle relaxation to achieve wrinkle removal and cosmetic effects. BTX-A is an ideal treatment for young beauty seekers who are unwilling to undergo surgery and do not want their treatment to interfere with their daily work. Botulinum toxin is a minimally invasive, convenient, safe, and reversible treatment for facial rejuvenation, but the effect is relatively short-lived. In general, functional recovery at the nerve-muscle gap gradually recovers to reinnervate target muscles within 3 to 6 months. Therefore, to maintain the effect, it is necessary to either reinject BTX-A every 6 months or seek other treatment options.
At present, there has been no systematic review of BTX-A in the treatment of neck wrinkles to our knowledge. Hence, we set out to discuss and review the pertinent clinical studies of BTX-A on neck wrinkles that evaluated its efficacy and safety.
MATERIALS AND METHODS
Search Strategy
Two investigators (H.Q. and R.Z.) independently performed a systematic search of the Web of Science, PubMed, EMBASE, Cochrane Library, and SCOPUS databases to identify all studies related to the utilization of BTX-A in neck wrinkles. We employed the following key words and/or corresponding medical subject heading terms: botulinum or botulinum toxin or Botox or botulin or botulinus toxin or botulinum toxin type A or onabotulinum toxin A or abobotulinum toxin A or incobotulinum toxin A; and neck wrinkles or neck lines or cervical stripe or neck aging or neck rejuvenation or neck contours. The search was conducted on April 30, 2020. The same 2 authors (H.Q. and R.Z.) conducted a preliminary screening of all article titles and abstracts to determine whether they met the inclusion criteria, and these same authors reviewed the search results and performed the data analysis. Disagreements were resolved through discussion with another author (S.L.). Further disagreement was settled by another senior author (H.W.). The study conforms to the Declaration of Helsinki. Figure 1 shows the selection process and exclusion criteria for the study.
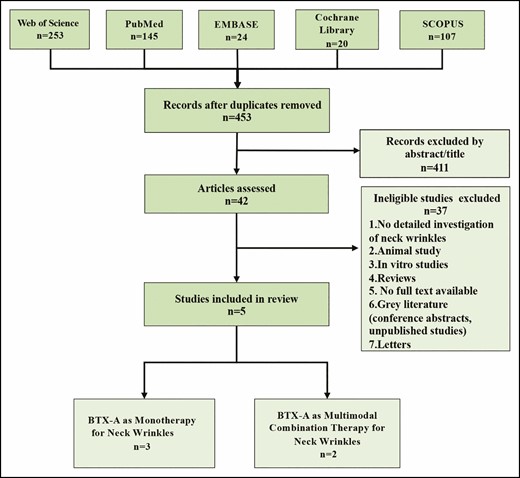
A flow diagram of the literature search and study selection process.
Eligibility Criteria
Referring to the PICOS principles commonly utilized worldwide, we specified the eligibility criteria for the patients as follows: (1) P (patients included in the study): all patients were plagued by neck wrinkles and sought related treatment; (2) I (intervention): single or combined injection of BTX-A; (3) C (control): all studies compared BTX-A with other interventions or a no-intervention control group; (4) O (outcomes): after treatment, the efficacy was observed during an average follow-up period of more than 2 weeks; and (5) S (study design): randomized controlled trials, retrospective cohorts, case-control studies, and prospective investigations. Because of the close relationship between the platysmal band and neck wrinkles, the specific evaluation of the results of neck wrinkles treated with BTX-A in the treatment of platysmal bands was also included in the review. Written informed consent was obtained from all participants.
RESULTS
In strict accordance with the pre-established retrieval strategy and the relevant inclusion and exclusion criteria, we selected 5 suitable studies with a total of 112 patients who underwent botulinum toxin injection for neck wrinkles.6-10 The patients were all female and aged from 24 to 65 years (mean age 46). The most obvious finding to emerge from this analysis was that, in addition to utilizing BTX-A as monotherapy, it can also be utilized in conjunction with other methods or in a topical cream to treat neck wrinkles. In the included studies, the formulations of BTX-A included prabotulinum toxin A (Daewoong Pharmaceutical Co. Ltd., Seoul, Korea), abobotulinum toxin A (Ipsen Ltd, Berks, UK), incobotulinum toxin A (Merz Pharmaceuticals GmbH, Frankfurt, Germany), and BTX-A cream (AbbVie Inc., North Chicago, IL). Efficacy was assessed employing the Investigator Global Aesthetic Improvement Scale, the Wrinkle Assessment Scale,6 and the subjective satisfaction of the patients, with follow-up assessments ranging from 3 days to 6 weeks (mean follow-up time: 54 days). Overall, the utilization of the BTX-A technique, with or without other neck rejuvenation approaches, permitted surgeons to fulfill the expectations of patients. The complication rate was negligible.
The patient clinical characteristics and outcomes of the included studies are presented in Table 1. Together, these results provide important insights into the treatment of neck wrinkles. The specific treatment details of the related studies, especially the formulations, dose, injection method, measurement method, follow-up time, and treatment effect of the BTX-A applied, are systematically summarized below to provide a theoretical basis and data support for further research in the future.
Studies Concerning the Treatment of Neck Wrinkles With BTX-A
| Refer- ence | Type of study | Intervention type | Sample size/age, y | Injected volume/ injection site | Scale | Follow-up period | Results |
|---|---|---|---|---|---|---|---|
| BTX-A as monotherapy for neck wrinkles | |||||||
| 6 | Prospective observational study | Prabotulinum toxin A (Nabota: Daewoong Pharmaceutical Co. Ltd., Seoul, Korea) | 20 (female)/ average 43 | Performed at points 1-1.5 cm apart along horizontal lines with 1-2 U in each injection site for total 15-30 U | Wrinkle Assessment Scale; Assessment of improvement of patient and satisfaction level | 3, 8 d and 1, 2, 3, 4 mo postopy | <50% improvement rate and satisfaction; 9 patients had minor adverse reactions; adverse reactions mild and transitory |
| 7 | Prospective crossover clinical trial | Abobotulinumtoxin A (Dysport; Ipsen Ltd, Berks, UK) | 30 (female)/average 55.9 | Mean dose of 154 U per patient with Microbotox technique; 150 injections delivered over entire anterior neck in an area | IGAIS; SGAIS; validated photonumeric scales | 15 d postop | 100% patients satisfied with results; Microbotox technique was greater than Nefertiti technique on improvement of mandible and neck volume but not for platysmal bands at rest or with contraction; 3 patients who received Microbotox technique had injection-point ecchymosis that disappeared in a couple of days |
| 8 | Single-center, single-blinded, parallel-group, prospective study | Topical BoNTA cream (CosmeTox, AbbVie Inc., North Chicago, IL) | 40 (female)/mean 49 ± 5 | Per patient dose during trial period: 50-70 U depending on treatment duration | Facial Wrinkle Scale; SGAIS; self-perception of age assessments | Once/wk until 12 wk or more postop | Although no analysis of related data for neck improvement, 100% of patients reported looking younger; 3 adverse events (tight feeling across forehead, pulling lines on upper outer eyelids, and dryness of area) occurred; no serious adverse events during entire study period |
| BTX-A as multimodal combination therapy for neck wrinkles | |||||||
| 9 | Prospective, evaluator-blinded study | Intensity focused ultrasound (Ulthera System; Ulthera, Inc., Mesa, AZ); CPMHA (Belotero Soft; Anteis SA, Geneva, Switzerland); Incobotulinum toxin A (Xeomin; Merz Pharmaceuticals GmbH, Frankfurt, Germany) | 12 (female)/ average 33.5 | Total dose of 40 U divided into approximately 40 injections spaced 1-2 cm apart in zigzag pattern along wrinkles | GAIS; 2-dimensional ultrasound; modified classification of horizontal neck wrinkles | Day 0 and 1; 2, 3, and 6 mo postop | 41.7% very satisfied, 41.7% satisfied, 8.3% slightly satisfied, and 8.3% unsatisfied with results at 6 mo posttreat; posttreat erythema and petechiae completely resolved within 14 d; no other side effects except CPMHA-induced lumps |
| 10 | Retrospective study | Microfocused ultrasound- visualization (Ulthera; Merz North America, Inc., Raleigh, NC); CPMHA (Belotero balance or Belotero soft; Merz North America, Inc.); Incobotulinum toxin A (Xeomin; Merz Pharmaceuticals) | 10 (female)/average 53.8 | Did not exceed 50 U per patient; 2 U injected intramuscularly into platysmal band every 2 cm; 0.5 U injected into subdermal area at 1-cm intervals above and below transverse neck line | Primary evaluation of photographs; Secondary evaluation of scoring Table 3 | Preop and 3 mo postop | 100% of patients showed clinical improvement in primary evaluation of efficacy; patients with worse initial status of neck aging and higher initial scores had better outcomes; no significant adverse reactions reported |
| Refer- ence | Type of study | Intervention type | Sample size/age, y | Injected volume/ injection site | Scale | Follow-up period | Results |
|---|---|---|---|---|---|---|---|
| BTX-A as monotherapy for neck wrinkles | |||||||
| 6 | Prospective observational study | Prabotulinum toxin A (Nabota: Daewoong Pharmaceutical Co. Ltd., Seoul, Korea) | 20 (female)/ average 43 | Performed at points 1-1.5 cm apart along horizontal lines with 1-2 U in each injection site for total 15-30 U | Wrinkle Assessment Scale; Assessment of improvement of patient and satisfaction level | 3, 8 d and 1, 2, 3, 4 mo postopy | <50% improvement rate and satisfaction; 9 patients had minor adverse reactions; adverse reactions mild and transitory |
| 7 | Prospective crossover clinical trial | Abobotulinumtoxin A (Dysport; Ipsen Ltd, Berks, UK) | 30 (female)/average 55.9 | Mean dose of 154 U per patient with Microbotox technique; 150 injections delivered over entire anterior neck in an area | IGAIS; SGAIS; validated photonumeric scales | 15 d postop | 100% patients satisfied with results; Microbotox technique was greater than Nefertiti technique on improvement of mandible and neck volume but not for platysmal bands at rest or with contraction; 3 patients who received Microbotox technique had injection-point ecchymosis that disappeared in a couple of days |
| 8 | Single-center, single-blinded, parallel-group, prospective study | Topical BoNTA cream (CosmeTox, AbbVie Inc., North Chicago, IL) | 40 (female)/mean 49 ± 5 | Per patient dose during trial period: 50-70 U depending on treatment duration | Facial Wrinkle Scale; SGAIS; self-perception of age assessments | Once/wk until 12 wk or more postop | Although no analysis of related data for neck improvement, 100% of patients reported looking younger; 3 adverse events (tight feeling across forehead, pulling lines on upper outer eyelids, and dryness of area) occurred; no serious adverse events during entire study period |
| BTX-A as multimodal combination therapy for neck wrinkles | |||||||
| 9 | Prospective, evaluator-blinded study | Intensity focused ultrasound (Ulthera System; Ulthera, Inc., Mesa, AZ); CPMHA (Belotero Soft; Anteis SA, Geneva, Switzerland); Incobotulinum toxin A (Xeomin; Merz Pharmaceuticals GmbH, Frankfurt, Germany) | 12 (female)/ average 33.5 | Total dose of 40 U divided into approximately 40 injections spaced 1-2 cm apart in zigzag pattern along wrinkles | GAIS; 2-dimensional ultrasound; modified classification of horizontal neck wrinkles | Day 0 and 1; 2, 3, and 6 mo postop | 41.7% very satisfied, 41.7% satisfied, 8.3% slightly satisfied, and 8.3% unsatisfied with results at 6 mo posttreat; posttreat erythema and petechiae completely resolved within 14 d; no other side effects except CPMHA-induced lumps |
| 10 | Retrospective study | Microfocused ultrasound- visualization (Ulthera; Merz North America, Inc., Raleigh, NC); CPMHA (Belotero balance or Belotero soft; Merz North America, Inc.); Incobotulinum toxin A (Xeomin; Merz Pharmaceuticals) | 10 (female)/average 53.8 | Did not exceed 50 U per patient; 2 U injected intramuscularly into platysmal band every 2 cm; 0.5 U injected into subdermal area at 1-cm intervals above and below transverse neck line | Primary evaluation of photographs; Secondary evaluation of scoring Table 3 | Preop and 3 mo postop | 100% of patients showed clinical improvement in primary evaluation of efficacy; patients with worse initial status of neck aging and higher initial scores had better outcomes; no significant adverse reactions reported |
CPMHA = Cohesive Polydensified Matrix Hyaluronic Acid; GAIS = Global Aesthetic Improvement Scale; IGAIS = Investigator Global Aesthetic Improvement Scale; preop = preoperatively; postop = postoperatively; posttreat, posttreatment; SGAIS = Subject Global Aesthetic Improvement Scale.
Studies Concerning the Treatment of Neck Wrinkles With BTX-A
| Refer- ence | Type of study | Intervention type | Sample size/age, y | Injected volume/ injection site | Scale | Follow-up period | Results |
|---|---|---|---|---|---|---|---|
| BTX-A as monotherapy for neck wrinkles | |||||||
| 6 | Prospective observational study | Prabotulinum toxin A (Nabota: Daewoong Pharmaceutical Co. Ltd., Seoul, Korea) | 20 (female)/ average 43 | Performed at points 1-1.5 cm apart along horizontal lines with 1-2 U in each injection site for total 15-30 U | Wrinkle Assessment Scale; Assessment of improvement of patient and satisfaction level | 3, 8 d and 1, 2, 3, 4 mo postopy | <50% improvement rate and satisfaction; 9 patients had minor adverse reactions; adverse reactions mild and transitory |
| 7 | Prospective crossover clinical trial | Abobotulinumtoxin A (Dysport; Ipsen Ltd, Berks, UK) | 30 (female)/average 55.9 | Mean dose of 154 U per patient with Microbotox technique; 150 injections delivered over entire anterior neck in an area | IGAIS; SGAIS; validated photonumeric scales | 15 d postop | 100% patients satisfied with results; Microbotox technique was greater than Nefertiti technique on improvement of mandible and neck volume but not for platysmal bands at rest or with contraction; 3 patients who received Microbotox technique had injection-point ecchymosis that disappeared in a couple of days |
| 8 | Single-center, single-blinded, parallel-group, prospective study | Topical BoNTA cream (CosmeTox, AbbVie Inc., North Chicago, IL) | 40 (female)/mean 49 ± 5 | Per patient dose during trial period: 50-70 U depending on treatment duration | Facial Wrinkle Scale; SGAIS; self-perception of age assessments | Once/wk until 12 wk or more postop | Although no analysis of related data for neck improvement, 100% of patients reported looking younger; 3 adverse events (tight feeling across forehead, pulling lines on upper outer eyelids, and dryness of area) occurred; no serious adverse events during entire study period |
| BTX-A as multimodal combination therapy for neck wrinkles | |||||||
| 9 | Prospective, evaluator-blinded study | Intensity focused ultrasound (Ulthera System; Ulthera, Inc., Mesa, AZ); CPMHA (Belotero Soft; Anteis SA, Geneva, Switzerland); Incobotulinum toxin A (Xeomin; Merz Pharmaceuticals GmbH, Frankfurt, Germany) | 12 (female)/ average 33.5 | Total dose of 40 U divided into approximately 40 injections spaced 1-2 cm apart in zigzag pattern along wrinkles | GAIS; 2-dimensional ultrasound; modified classification of horizontal neck wrinkles | Day 0 and 1; 2, 3, and 6 mo postop | 41.7% very satisfied, 41.7% satisfied, 8.3% slightly satisfied, and 8.3% unsatisfied with results at 6 mo posttreat; posttreat erythema and petechiae completely resolved within 14 d; no other side effects except CPMHA-induced lumps |
| 10 | Retrospective study | Microfocused ultrasound- visualization (Ulthera; Merz North America, Inc., Raleigh, NC); CPMHA (Belotero balance or Belotero soft; Merz North America, Inc.); Incobotulinum toxin A (Xeomin; Merz Pharmaceuticals) | 10 (female)/average 53.8 | Did not exceed 50 U per patient; 2 U injected intramuscularly into platysmal band every 2 cm; 0.5 U injected into subdermal area at 1-cm intervals above and below transverse neck line | Primary evaluation of photographs; Secondary evaluation of scoring Table 3 | Preop and 3 mo postop | 100% of patients showed clinical improvement in primary evaluation of efficacy; patients with worse initial status of neck aging and higher initial scores had better outcomes; no significant adverse reactions reported |
| Refer- ence | Type of study | Intervention type | Sample size/age, y | Injected volume/ injection site | Scale | Follow-up period | Results |
|---|---|---|---|---|---|---|---|
| BTX-A as monotherapy for neck wrinkles | |||||||
| 6 | Prospective observational study | Prabotulinum toxin A (Nabota: Daewoong Pharmaceutical Co. Ltd., Seoul, Korea) | 20 (female)/ average 43 | Performed at points 1-1.5 cm apart along horizontal lines with 1-2 U in each injection site for total 15-30 U | Wrinkle Assessment Scale; Assessment of improvement of patient and satisfaction level | 3, 8 d and 1, 2, 3, 4 mo postopy | <50% improvement rate and satisfaction; 9 patients had minor adverse reactions; adverse reactions mild and transitory |
| 7 | Prospective crossover clinical trial | Abobotulinumtoxin A (Dysport; Ipsen Ltd, Berks, UK) | 30 (female)/average 55.9 | Mean dose of 154 U per patient with Microbotox technique; 150 injections delivered over entire anterior neck in an area | IGAIS; SGAIS; validated photonumeric scales | 15 d postop | 100% patients satisfied with results; Microbotox technique was greater than Nefertiti technique on improvement of mandible and neck volume but not for platysmal bands at rest or with contraction; 3 patients who received Microbotox technique had injection-point ecchymosis that disappeared in a couple of days |
| 8 | Single-center, single-blinded, parallel-group, prospective study | Topical BoNTA cream (CosmeTox, AbbVie Inc., North Chicago, IL) | 40 (female)/mean 49 ± 5 | Per patient dose during trial period: 50-70 U depending on treatment duration | Facial Wrinkle Scale; SGAIS; self-perception of age assessments | Once/wk until 12 wk or more postop | Although no analysis of related data for neck improvement, 100% of patients reported looking younger; 3 adverse events (tight feeling across forehead, pulling lines on upper outer eyelids, and dryness of area) occurred; no serious adverse events during entire study period |
| BTX-A as multimodal combination therapy for neck wrinkles | |||||||
| 9 | Prospective, evaluator-blinded study | Intensity focused ultrasound (Ulthera System; Ulthera, Inc., Mesa, AZ); CPMHA (Belotero Soft; Anteis SA, Geneva, Switzerland); Incobotulinum toxin A (Xeomin; Merz Pharmaceuticals GmbH, Frankfurt, Germany) | 12 (female)/ average 33.5 | Total dose of 40 U divided into approximately 40 injections spaced 1-2 cm apart in zigzag pattern along wrinkles | GAIS; 2-dimensional ultrasound; modified classification of horizontal neck wrinkles | Day 0 and 1; 2, 3, and 6 mo postop | 41.7% very satisfied, 41.7% satisfied, 8.3% slightly satisfied, and 8.3% unsatisfied with results at 6 mo posttreat; posttreat erythema and petechiae completely resolved within 14 d; no other side effects except CPMHA-induced lumps |
| 10 | Retrospective study | Microfocused ultrasound- visualization (Ulthera; Merz North America, Inc., Raleigh, NC); CPMHA (Belotero balance or Belotero soft; Merz North America, Inc.); Incobotulinum toxin A (Xeomin; Merz Pharmaceuticals) | 10 (female)/average 53.8 | Did not exceed 50 U per patient; 2 U injected intramuscularly into platysmal band every 2 cm; 0.5 U injected into subdermal area at 1-cm intervals above and below transverse neck line | Primary evaluation of photographs; Secondary evaluation of scoring Table 3 | Preop and 3 mo postop | 100% of patients showed clinical improvement in primary evaluation of efficacy; patients with worse initial status of neck aging and higher initial scores had better outcomes; no significant adverse reactions reported |
CPMHA = Cohesive Polydensified Matrix Hyaluronic Acid; GAIS = Global Aesthetic Improvement Scale; IGAIS = Investigator Global Aesthetic Improvement Scale; preop = preoperatively; postop = postoperatively; posttreat, posttreatment; SGAIS = Subject Global Aesthetic Improvement Scale.
BTX-A as Monotherapy for Neck Wrinkles
Three studies reported the effects of BTX-A treatment as monotherapy on neck wrinkles.6-8 A total of 90 patients were enrolled, and all of them were women with an average age of 50 years. No serious adverse reactions were found during the follow-up period. The satisfaction level of treated patients was high to a certain extent. Due to the contraction of sweat glands or sebaceous glands from the intradermal effect, the texture of the skin was also improved to some extent.
The dermal, subdermal, or intramuscular levels are often the conventional target structures of botulinum toxin. Interestingly, Wu11 first proposed the MicroBotox technology to improve forehead wrinkles in 2001, and this approach has gradually gained popularity in lower face and neck rejuvenation. The core point is the multiple microdroplets of diluted BTX-A distributed over a large area in the dermis or just beyond, which relaxes the superficial muscle fibers and does not eliminate the deep fiber function of the muscle but obtains a lifting, tightening, and smoother skin appearance.12,13 What is the effect of applying MicroBotox technology in the neck? Dr Wu,7 the pioneer of the MicroBotox technique, maintains that this technique can produce optimal outcomes for horizontal neck creases. In studies conducted by Wu,11 it was shown that each 1-mL syringe of MicroBotox solution contains 20 to 28 units of BTX-A, and 1 mL is recommended for the lower face and unilateral neck injection. Conversely, Steven Liew12 reported no significant difference in deep horizontal creases. MicroBotox injection can improve superficial neck wrinkles but is ineffective for deep wrinkles because the superficial muscle is attached to the dermis. Due to the injection of a large area and shallow skin layer, it is difficult to control pain with this approach, which limits the popularization of this technique. A superficial injection needling botulinum technique developed by Francesco Calvani14 currently exists for dermal hyperconcentrated injection of multiple microdroplets by electrical devices, unlike the hyperdiluted injection of the MicroBotox technique. The same researchers adopted this technique to show improvement in face and neck wrinkles. Taken together, these studies support the notion that the injection of botulin toxin into the dermis or in the subdermal plane may be a recommended alternative. Notably, the MicroBotox technique is more effective on soft tissue ptosis than the Nefertiti technique,15,16 which is more effective on platysmal bands.7 The main characteristics of the MicroBotox and the Nefertiti Lift are summarized in Table 2.
The Main Characteristics of the MicroBotox and the “Nefertiti Lift”
| MicroBotox | Nefertiti lift | |
|---|---|---|
| Historical context | First developed by Wu in 2001.11 MicroBotox, initially called “mesobotox,” delivers multiple diluted BTX-A into overlying skin envelope and superficial layer of facial and neck muscles | Levy first described in 2007.15 Focuses specifically on platysmal bands and inferior border of mandible with BTX-A |
| Injection effect | To specifically decrease sweat and sebaceous gland activity to improve skin texture, shrink pores, and enhance sheen. MicroBotox targets superficial fibers of skin to smooth fine lines and wrinkles on face and neck and achieve better contour while not eliminating function of the deep fibers12 | Creates visual effect of a “mini lift” by specifically lifting corners of the mouth, recontouring mandibular border and angle, and elevating skin at jawline |
| Indication | Predominant soft tissue ptosis in lower face and neck7 | Predominant platysmal hyperactivity and minor soft tissue ptosis7 |
| Injection technique | Injecting microdroplets of 0.003 to 0.005 mL to dermis and subdermis using 1-mL syringe and 30-gauge needle at 0.8- to 1-cm intervals. 100-150 injections done into superficial dermis over entire anterior neck, corresponding to extent of platysmal muscle13 | At the back of the hypothetical line where nasolabial fold passes through mandible, injections are administered s.c. at 1- to 2- cm intervals using 30-gauge needle and 1-mL syringe along horizontal line below edge of mandible. Platysma muscle band held between thumb and index finger of nondominant hand and injected i.m. along platysma muscle band at interval of 2 cm16 |
| Complication | Can prevent toxin from spreading unnecessarily to deep structure of the neck, minimizing risk of adverse events such as dysphonia, dysphagia, and neck muscle weakness. | More likely to migrate into surrounding deep muscles at higher doses compared with MicroBotox technique |
| MicroBotox | Nefertiti lift | |
|---|---|---|
| Historical context | First developed by Wu in 2001.11 MicroBotox, initially called “mesobotox,” delivers multiple diluted BTX-A into overlying skin envelope and superficial layer of facial and neck muscles | Levy first described in 2007.15 Focuses specifically on platysmal bands and inferior border of mandible with BTX-A |
| Injection effect | To specifically decrease sweat and sebaceous gland activity to improve skin texture, shrink pores, and enhance sheen. MicroBotox targets superficial fibers of skin to smooth fine lines and wrinkles on face and neck and achieve better contour while not eliminating function of the deep fibers12 | Creates visual effect of a “mini lift” by specifically lifting corners of the mouth, recontouring mandibular border and angle, and elevating skin at jawline |
| Indication | Predominant soft tissue ptosis in lower face and neck7 | Predominant platysmal hyperactivity and minor soft tissue ptosis7 |
| Injection technique | Injecting microdroplets of 0.003 to 0.005 mL to dermis and subdermis using 1-mL syringe and 30-gauge needle at 0.8- to 1-cm intervals. 100-150 injections done into superficial dermis over entire anterior neck, corresponding to extent of platysmal muscle13 | At the back of the hypothetical line where nasolabial fold passes through mandible, injections are administered s.c. at 1- to 2- cm intervals using 30-gauge needle and 1-mL syringe along horizontal line below edge of mandible. Platysma muscle band held between thumb and index finger of nondominant hand and injected i.m. along platysma muscle band at interval of 2 cm16 |
| Complication | Can prevent toxin from spreading unnecessarily to deep structure of the neck, minimizing risk of adverse events such as dysphonia, dysphagia, and neck muscle weakness. | More likely to migrate into surrounding deep muscles at higher doses compared with MicroBotox technique |
BTX-A = botulinum toxin A; i.m. = intramuscularly; s.c. = subcutaneously.
The Main Characteristics of the MicroBotox and the “Nefertiti Lift”
| MicroBotox | Nefertiti lift | |
|---|---|---|
| Historical context | First developed by Wu in 2001.11 MicroBotox, initially called “mesobotox,” delivers multiple diluted BTX-A into overlying skin envelope and superficial layer of facial and neck muscles | Levy first described in 2007.15 Focuses specifically on platysmal bands and inferior border of mandible with BTX-A |
| Injection effect | To specifically decrease sweat and sebaceous gland activity to improve skin texture, shrink pores, and enhance sheen. MicroBotox targets superficial fibers of skin to smooth fine lines and wrinkles on face and neck and achieve better contour while not eliminating function of the deep fibers12 | Creates visual effect of a “mini lift” by specifically lifting corners of the mouth, recontouring mandibular border and angle, and elevating skin at jawline |
| Indication | Predominant soft tissue ptosis in lower face and neck7 | Predominant platysmal hyperactivity and minor soft tissue ptosis7 |
| Injection technique | Injecting microdroplets of 0.003 to 0.005 mL to dermis and subdermis using 1-mL syringe and 30-gauge needle at 0.8- to 1-cm intervals. 100-150 injections done into superficial dermis over entire anterior neck, corresponding to extent of platysmal muscle13 | At the back of the hypothetical line where nasolabial fold passes through mandible, injections are administered s.c. at 1- to 2- cm intervals using 30-gauge needle and 1-mL syringe along horizontal line below edge of mandible. Platysma muscle band held between thumb and index finger of nondominant hand and injected i.m. along platysma muscle band at interval of 2 cm16 |
| Complication | Can prevent toxin from spreading unnecessarily to deep structure of the neck, minimizing risk of adverse events such as dysphonia, dysphagia, and neck muscle weakness. | More likely to migrate into surrounding deep muscles at higher doses compared with MicroBotox technique |
| MicroBotox | Nefertiti lift | |
|---|---|---|
| Historical context | First developed by Wu in 2001.11 MicroBotox, initially called “mesobotox,” delivers multiple diluted BTX-A into overlying skin envelope and superficial layer of facial and neck muscles | Levy first described in 2007.15 Focuses specifically on platysmal bands and inferior border of mandible with BTX-A |
| Injection effect | To specifically decrease sweat and sebaceous gland activity to improve skin texture, shrink pores, and enhance sheen. MicroBotox targets superficial fibers of skin to smooth fine lines and wrinkles on face and neck and achieve better contour while not eliminating function of the deep fibers12 | Creates visual effect of a “mini lift” by specifically lifting corners of the mouth, recontouring mandibular border and angle, and elevating skin at jawline |
| Indication | Predominant soft tissue ptosis in lower face and neck7 | Predominant platysmal hyperactivity and minor soft tissue ptosis7 |
| Injection technique | Injecting microdroplets of 0.003 to 0.005 mL to dermis and subdermis using 1-mL syringe and 30-gauge needle at 0.8- to 1-cm intervals. 100-150 injections done into superficial dermis over entire anterior neck, corresponding to extent of platysmal muscle13 | At the back of the hypothetical line where nasolabial fold passes through mandible, injections are administered s.c. at 1- to 2- cm intervals using 30-gauge needle and 1-mL syringe along horizontal line below edge of mandible. Platysma muscle band held between thumb and index finger of nondominant hand and injected i.m. along platysma muscle band at interval of 2 cm16 |
| Complication | Can prevent toxin from spreading unnecessarily to deep structure of the neck, minimizing risk of adverse events such as dysphonia, dysphagia, and neck muscle weakness. | More likely to migrate into surrounding deep muscles at higher doses compared with MicroBotox technique |
BTX-A = botulinum toxin A; i.m. = intramuscularly; s.c. = subcutaneously.
In addition, a novel topical BTX-A cream (CosmeTox) for treating hyperfunctional wrinkles of neck areas has attracted our attention.8 The study was limited by the lack of information on the evaluation of neck improvement. Despite this limitation, this study certainly offers some insight into a novel therapy. For those who suffer from a needle phobia, or for maintenance therapy to prolong the effect of BTX-A, this novel topical treatment may be a pain-free, needle-free method to receive BTX-A treatment. Taken together, these results provide a basis for the therapeutic effects of BTX-A in neck wrinkles.
BTX-A as Multimodal Combination Therapy for Neck Wrinkles
There were only 2 reports about multimodal combination therapy, and the average age of the 22 female patients was 39.7 years. The combination therapy is mainly ultrasound therapy, skin fillers, and botulinum toxin, which play different roles and complement each other. The valid results can last for 6 months. In 2018, Jeon9 reported a 1-day multimodal treatment with the sequence of intensity focused ultrasound, cohesive polydensified matrix hyaluronic acid, and incobotulinum toxin A in the same clinic setting. Ten Korean patients also received a single-day session of 3 kinds of interventions in a single dermatology clinic to restore skin laxity, fill missing volume, and relax the platysmal bands.10 In this retrospective study, incobotulinum toxin A was injected along the platysmal bands and above and below the horizontal neck lines while the hyaluronic acid filler was injected along the lines immediately after microfocused ultrasound with visualization (MFU-V). MFU-V is effective in treating mild to moderate skin relaxation, especially submental fat that is easy to ignore, and it is effective for Asians after the age of 40 years. The transverse wrinkle of the neck shows a sunken strip texture, and the strip texture caused by the contraction of the platysma muscle is often shown as a longitudinal wrinkle. In the combined treatment of neck wrinkles, researchers often choose hyaluronic acid to fill sunken wrinkles combined with BTX-A to improve platysmal-caused wrinkles. The cohesive polydensified matrix hyaluronic acid (Belotero soft; Anteis SA, Geneva, Switzerland) utilized in the published literature is a cross-linked hyaluronic acid to fill superficial wrinkles. It is worth mentioning that, due to the thin skin of the neck, the horizontal wrinkles often manifest as fine and superficial characteristics, and the non–cross-linked hyaluronic acid preparation can eliminate the nodule, an unsightly beading appearance and skin irregularity phenomenon produced by the cross-linked, polydensified preparation. Recently, hyaluronic acid fillers with low viscosity and elasticity were expected to be one of the most effective preparations utilized to restore soft tissue volume due to their properties of being soft and easily molded.17 However, the effect of the maintenance time, viscosity, and injection placement of the non–cross-linked preparation should be taken into consideration.18 Two methods of clinical evaluations were carried out 3 months after the operation, and the results showed that there was a statistically significant difference in transverse line scores before and after treatment, and the patients with a poor initial state of neck aging and a high initial score had the best improvement after treatment. In view of the action mechanism of different treatment methods and the multiple factors of neck lines, an increasing number of researchers tend to combine a variety of intervention measures, often achieving satisfactory and lasting results.
Complications
The most common side effects were pain, hematoma, ecchymosis, and bruising. Fortunately, most of these side effects were mild and short-lived and disappeared spontaneously. Serious potential adverse events, such as dysphonia, dysphagia, and neck weakness, were often related to functional imbalance in extended aesthetic utilization of BTX-A, especially the extended area of the neck. Of note, a case reported by Phothong et al19 presented adverse effects of BTX-A injection for the treatment of platysmal bands. A 47-year-old Thai woman suffered dysphagia after receiving a 70-IU injection of BTX-A along the anterior and both lateral sides of the neck. The platysma muscle maintains a complicated anatomical relationship with the functional neck muscle, so a comprehensive anatomical and physiological understanding of the platysma and its related muscles will facilitate neck rejuvenation. For the treatment of vertical or horizontal neck lines, the recommended dose is limited to 25 to 30 per cervical Botox treatment session for a maximum total dose of 60 U.20 For other types of preparations, there is dose inequality and noninterchangeability in clinical utilization. As noted by Alan Matarasso, 21,22 the degree of muscle relaxation, muscle hypertrophy, muscle length, and degree of sagginess of the overlying skin should be included in the guidelines for dosages of botulinum for the management of platysmal bands. In combination therapy, the possible complications of other treatments should not be underestimated. A study reported several cases illustrating a rare adverse reaction induced by microimplants in the treatment of neck wrinkles.23 Chajchir et al8 systematically classified the potential complications into 3 categories: relative, descriptive, and rare. Nonstandard preparation of the toxin, improper selection of the dose, incorrect injection techniques, lack of a postinjection protocol, lack of understanding of anatomy, and individual specificity of patients may be risk factors for complications.
Discussion
There are various surgical and nonsurgical techniques utilized alone or in combination to address the aging process of the neck and to achieve long-term neck rejuvenation results.24 Compared with traditional surgery, minimally invasive treatment is simple and rapid, is less invasive with virtually no down time, and the recovery effect is more natural. Many cosmetic treatments exist to address neck wrinkles, including local skin tissue fillers, lasers, radiofrequency energy, intradermal neuromodulator injection, or thread lifting, as shown in Table 3. Topical drugs are also effective methods.25 Soft tissue fillers such as hyaluronic acid,26-29 polylactic acid,30 calcium hydroxyapatite,31 and adipose tissue32 mainly physically fill the neck tissue volume loss, supplement skin volume, or stimulate skin tissue regeneration and relieve moderate wrinkles. Intradermal radiofrequency,33 thread lift implantation,34 microfocused ultrasound,35,36 and lasers37,38 lead to similar functional effects in stimulating the local skin tissue to reshape collagen and tighten the skin, but they have little effect on reducing rhytides. Although there is a lack of sufficient systematic research, platelet concentrated products,39 mesoderm therapy,40 and autologous keratin and fibroblasts41 show great application prospects in the treatment of neck wrinkles. The neuromodulators of botulinum toxin, especially BTX-A, have shown great usefulness in the attenuation of wrinkles of the neck region.6-8
Relevant Minimally Invasive Treatments for Neck Wrinkles
| Therapy | References | Neck wrinkle condition of the patients | Functional effects | |
|---|---|---|---|---|
| BTX-A | 6-8 | Mild to moderate | Reduce platysmal bands and marginally improve neck lines | |
| Skin tissue filler | Hyaluronic acid | 26-29 | Mild to moderate | Restore soft tissue volume |
| Polylactic acid | 30 | Not mentioned | Stimulate fibroblasts to proliferate and secrete collagen | |
| Calcium hydroxyapatite | 31 | Class I-III (Dedo’s classification system) | Dual-function filler intended to volumize immediately and then stimulate neocollagenesis through local fibrohistiocytic response | |
| Stromal vascular fraction gel | 32 | Mild to deep | Increase the collagen density of neck wrinkles | |
| Intradermal radiofrequency | 33 | Not mentioned | Nonablative skin rejuvenation through its thermal effects | |
| Thread lift implantation | 34 | Shallow to moderately deep | Stimulate fibroblast, collagenization, and neoangiogenesis to improve skin texture and laxity | |
| Microfocused ultrasound | 35,36 | Moderate to severe | Tighten and lift lax neck skin | |
| Laser treatment | 37,38 | Mild to moderate | Improve skin texture and neck laxity, nonablative skin remodeling of neck lines | |
| Platelet-rich plasma | 39 | Not mentioned | Improve micropigmentation, skin texture, and skin homogeneity | |
| Mesoderm therapy | 40 | Not mentioned | Promote collagen regeneration and improve tightness and smoothness of neck skin | |
| Autologous keratin and fibroblast | 41 | Mild to severe | Support tissue scaffolds and continuous secretion collagen |
| Therapy | References | Neck wrinkle condition of the patients | Functional effects | |
|---|---|---|---|---|
| BTX-A | 6-8 | Mild to moderate | Reduce platysmal bands and marginally improve neck lines | |
| Skin tissue filler | Hyaluronic acid | 26-29 | Mild to moderate | Restore soft tissue volume |
| Polylactic acid | 30 | Not mentioned | Stimulate fibroblasts to proliferate and secrete collagen | |
| Calcium hydroxyapatite | 31 | Class I-III (Dedo’s classification system) | Dual-function filler intended to volumize immediately and then stimulate neocollagenesis through local fibrohistiocytic response | |
| Stromal vascular fraction gel | 32 | Mild to deep | Increase the collagen density of neck wrinkles | |
| Intradermal radiofrequency | 33 | Not mentioned | Nonablative skin rejuvenation through its thermal effects | |
| Thread lift implantation | 34 | Shallow to moderately deep | Stimulate fibroblast, collagenization, and neoangiogenesis to improve skin texture and laxity | |
| Microfocused ultrasound | 35,36 | Moderate to severe | Tighten and lift lax neck skin | |
| Laser treatment | 37,38 | Mild to moderate | Improve skin texture and neck laxity, nonablative skin remodeling of neck lines | |
| Platelet-rich plasma | 39 | Not mentioned | Improve micropigmentation, skin texture, and skin homogeneity | |
| Mesoderm therapy | 40 | Not mentioned | Promote collagen regeneration and improve tightness and smoothness of neck skin | |
| Autologous keratin and fibroblast | 41 | Mild to severe | Support tissue scaffolds and continuous secretion collagen |
BTX-A = botulinum toxin A.
Relevant Minimally Invasive Treatments for Neck Wrinkles
| Therapy | References | Neck wrinkle condition of the patients | Functional effects | |
|---|---|---|---|---|
| BTX-A | 6-8 | Mild to moderate | Reduce platysmal bands and marginally improve neck lines | |
| Skin tissue filler | Hyaluronic acid | 26-29 | Mild to moderate | Restore soft tissue volume |
| Polylactic acid | 30 | Not mentioned | Stimulate fibroblasts to proliferate and secrete collagen | |
| Calcium hydroxyapatite | 31 | Class I-III (Dedo’s classification system) | Dual-function filler intended to volumize immediately and then stimulate neocollagenesis through local fibrohistiocytic response | |
| Stromal vascular fraction gel | 32 | Mild to deep | Increase the collagen density of neck wrinkles | |
| Intradermal radiofrequency | 33 | Not mentioned | Nonablative skin rejuvenation through its thermal effects | |
| Thread lift implantation | 34 | Shallow to moderately deep | Stimulate fibroblast, collagenization, and neoangiogenesis to improve skin texture and laxity | |
| Microfocused ultrasound | 35,36 | Moderate to severe | Tighten and lift lax neck skin | |
| Laser treatment | 37,38 | Mild to moderate | Improve skin texture and neck laxity, nonablative skin remodeling of neck lines | |
| Platelet-rich plasma | 39 | Not mentioned | Improve micropigmentation, skin texture, and skin homogeneity | |
| Mesoderm therapy | 40 | Not mentioned | Promote collagen regeneration and improve tightness and smoothness of neck skin | |
| Autologous keratin and fibroblast | 41 | Mild to severe | Support tissue scaffolds and continuous secretion collagen |
| Therapy | References | Neck wrinkle condition of the patients | Functional effects | |
|---|---|---|---|---|
| BTX-A | 6-8 | Mild to moderate | Reduce platysmal bands and marginally improve neck lines | |
| Skin tissue filler | Hyaluronic acid | 26-29 | Mild to moderate | Restore soft tissue volume |
| Polylactic acid | 30 | Not mentioned | Stimulate fibroblasts to proliferate and secrete collagen | |
| Calcium hydroxyapatite | 31 | Class I-III (Dedo’s classification system) | Dual-function filler intended to volumize immediately and then stimulate neocollagenesis through local fibrohistiocytic response | |
| Stromal vascular fraction gel | 32 | Mild to deep | Increase the collagen density of neck wrinkles | |
| Intradermal radiofrequency | 33 | Not mentioned | Nonablative skin rejuvenation through its thermal effects | |
| Thread lift implantation | 34 | Shallow to moderately deep | Stimulate fibroblast, collagenization, and neoangiogenesis to improve skin texture and laxity | |
| Microfocused ultrasound | 35,36 | Moderate to severe | Tighten and lift lax neck skin | |
| Laser treatment | 37,38 | Mild to moderate | Improve skin texture and neck laxity, nonablative skin remodeling of neck lines | |
| Platelet-rich plasma | 39 | Not mentioned | Improve micropigmentation, skin texture, and skin homogeneity | |
| Mesoderm therapy | 40 | Not mentioned | Promote collagen regeneration and improve tightness and smoothness of neck skin | |
| Autologous keratin and fibroblast | 41 | Mild to severe | Support tissue scaffolds and continuous secretion collagen |
BTX-A = botulinum toxin A.
The application of botulinum toxin in the field of aesthetic medicine has exceeded that of hyaluronic acid,42 becoming the most popular nonsurgical procedure. Since the birth of Botox, the first type of BTX-A in the world, other botulinum toxin formulations have also emerged. However, different types of preparations have different profiles of efficacy and safety, and the potency units of each preparation are not interchangeable.43 Judging from the reported literature, certain preparations of BTX-A have unique injection parameters.
The tension and shape of the platysma muscle and the ability of the platysma muscle to support the adipose tissue are paramount in the shape of the neck. The medial or lateral, single or multiple prominent vertical platysmal bands form the characteristics of aging neck aesthetics,24 presenting either in isolation or with other senescent neck changes concerning skin laxity, the accumulation of subcutaneous fat, and neck lines. The middle third of the platysma muscle is mainly responsible for horizontal neck wrinkles by pulling the neck skin towards the center. An Italian consensus report recommends a guideline on the aesthetic utilization of onabotulinum toxin A in the neck.44 We have recommended BTX-A injection alone as an appropriate practice for patients with isolated hypertrophic platysmal bands who retain skin elasticity and minimal submental fat.45 Botulinum toxin can chemically denervate the platysma muscle to lessen some of the exerted tension and reduce some of the wrinkling and banding produced by it, but the effect on the horizontal neck line is still limited. The relationship between the platysmal band and skin relaxation is still controversial.46 The Facial Aesthetics Consensus Group Faculty reported in 2008 that 27% of the faculty utilized neuromodulators to treat horizontal neck lines.47
We found that these studies were mostly performed on female patients. However, there is an increasing trend of more men seeking to achieve neck aesthetic improvements. Evaluation and treatment of the aging neck would be better if they were individualized. Mastering the important differences between male and female patients enables plastic surgeons to appropriately address and correct patient aesthetic concerns, achieving consistent and reliable results. In the included studies, we also learned that the evaluation of neck lines was mainly based on the 5-point Global Aesthetic Improvement Scale, the satisfaction level of patients, or other evaluation methods. Patients’ subjective evaluation is often different from the actual situation. After all, the differences in subjective and objective evaluation between evaluators and beauty seekers may often lead to a patient’s unpleasant medical experience. Recently, a 5-point Photonumeric Allergan Transverse Neck Lines Scale was developed.48 It may serve as a validated and reliable scale for evaluating the severity of neck lines in daily clinical practice or future clinical studies, yet it is not suitable for rating vertical neck lines. The issue of scale is an intriguing one that could be usefully explored in further research. The follow-up time of monotherapy was at most only 4 months, but after combined treatment, the effect lasted for 24 weeks or more, which was consistent with other reports. The results suggest that BTX-A effectively limits muscle movement, reduces the absorption of hyaluronic acid fillers, alleviates the depth of wrinkles, delays maintenance time, and improves safety during treatment. It is important to mention that BTX-A has been traditionally administered by syringes in cosmetic applications. The microneedle approach, as mentioned before, has a number of attractive features: an ability to adjust the depth setting, hardly any recuperation time, multiplication of fibroblasts, synthesis of collagen and elastin, and dual effects acting on the sebaceous glands and muscles. Thus, the microneedling technique is a safe and outstanding innovation for the optimization of transdermal therapy in the attenuation of wrinkles of the neck region.
The aging of the neck is a multifactor process that usually requires a multimodal solution. There are many cosmetic methods for rejuvenating the neck, though published studies rarely reported the combination of multiple procedures. For multimodal approaches, we should take into account the timing and sequence of the BTX-A procedure. Two articles on multimodal therapy included in this paper had no significant differences between the sequence: BTX-A was immediately injected after treatment with MFU-V or intensity focused ultrasound, and hyaluronic acid was injected during the same course of treatment. BTX-A played the same role for platysmal bands as it did in monotherapy. Some scholars note that BTX-A should be injected 2 weeks before other treatments to avoid unwanted diffusion or after the local postoperative reactions caused by other approaches disappear. To achieve long-term aesthetic outcomes, we have to also take into account the bone structure, skin, blood vessels, and other factors that affect aging when treating neck wrinkles. However, few researchers have been able to draw on any systematic research into the field of multimodal combination therapy. Notwithstanding these limitations, further research is needed to more closely examine the efficacy and safety of BTX-A both as monotherapy and combined with other methods.
The face, neck and shoulders as a whole, as well as the influence of other parts, should not be ignored when the outline of 1 part is adjusted. Therefore, to obtain the perfect shape of the neck, multisite injection is often needed to achieve a harmonious and beautiful effect. Neck-related anatomy, details of injection location and BTX-A technique, total dose and unit injection dose of different products, evaluation indicators, and other variables (such as sex, age, race, etc) all have an impact on the outcome of neck wrinkle treatment.
Overall, these findings strengthen the idea that BTX-A can restore mild to moderate horizontal neck lines and smooth out the skin in the area where it is utilized. Unfortunately, BTX-A injections alone cannot achieve satisfactory results for severe wrinkles, which sometimes even require surgery. Furthermore, the effect is only a temporary improvement, similar to the experience of facial treatments with BTX-A. It must be admitted that the present study has some limitations. Because the included study was limited to a small sample size and short follow-up time, it was not possible to obtain a complete and systematic consensus on BTX-A injection for horizontal neck wrinkles. At present, there are few reports on the utilization of botulinum toxin in neck wrinkles at home and abroad. In fact, the prevalence rate of neck wrinkles is high, and the population is getting younger. Due to the minimal impact of BTX-A on the quality of life of patients, the consultation rate is often low. Furthermore, the current publications regarding BTX-A treatment of neck wrinkles are low-level evidence. The injection technique and evaluation methods of the published studies are diversified, which makes it difficult to perform comparisons between studies. Although the literature regarding neck wrinkles is mounting, an apparent lack of a unified description of the specific severity of neck wrinkles poses a limitation to a standard assessment of patient improvement rates as well as satisfaction. Lastly, whether the formation of neck wrinkles is related to region, race, and so on has not been determined, so the results of this study cannot provide adequate treatment evidence for clinical trials of specific populations. Despite the limitations of our review, this article is the first, to our knowledge, to systematically evaluate the aesthetic concerns of BTX-A in the treatment of neck wrinkles that is often of interest to many surgeons.
Conclusions
BTX-A, as a novel rejuvenation technology, is increasingly gaining in popularity in aesthetic neck rejuvenation. It can be utilized as monotherapy or in combination with other neck wrinkle procedures. However, there is a lack of large randomized controlled trials on this issue to provide more definitive evidence for the efficacy and safety of BTX-A for the treatment of neck wrinkles.
Acknowledgments
The authors acknowledge the valuable insights and timely help provided by the relevant people in conducting this literature search and review.
Disclosures
None of the authors has a financial interest in any of the products, devices, or drugs mentioned in this work.
Funding
The authors received no financial support for the research, authorship, or publication of this article.
References


{kind=link}