





Often diagnosed as an incidental finding during implant exchange or removal, double capsules are significantly more prevalent than initially supposed. Because many facets of pathogenesis, clinical recognition, and prevention remain to be elucidated, we laud the authors of “Defining Double Capsules: A Clinical and Histological Study” 1 for their work on this topic.
In this study, Van Slyke et al report on the presence of double capsules in 16 out of 22 consecutive Biocell (Allergan, Inc., Irvine, CA) implants removed or exchanged in an aesthetic practice. It was found that all areas of nonadherence of the macrotextured device were associated with double capsule formation, both clinically and histologically. Partial or complete double capsules were equally represented in the specimens, leading the authors to invoke the possibility of a spectrum of presentations from nascent capsules to a well-formed inner layer of double capsule. Their findings support the mechanical shear hypothesis postulated by previous studies.2,3
Various hypotheses for the etiology of double capsule formation were previously described by our team in 2015.4 The idea that a large implant pocket fails to firmly stabilize the implant leading to secondary formation of the inner capsule was refuted by findings demonstrating a “Velcro” effect by peeling of the internal capsule, which indicates that the initial capsule is still in contact with the prosthesis (Figure 1). Furthermore, a sterile intercapsular space was found by scanning electron microscopy (Figure 2), where one would have expected to find similar bacterial flora as that found on the surface of macrotextured implants according to the theory that the inner capsule forms secondarily. Similarly, the existence of mechanical shear stresses with chronic seromas, hematomas, or exudates subsequently leading to nascent inner layer formation cannot explain why the intercapsular spaces of double capsules were all sterile.
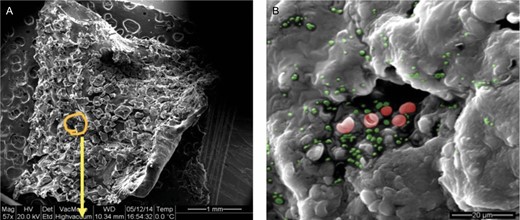
(A) Specimen obtained from peeling off the “Velcro” effect of the inner layer of a double capsule as seen under scanning electron microscopy at 57× magnification. (B) Demonstration of the presence of bacteria as clusters (red and green) seen under scanning electron microscopy at 400× magnification.
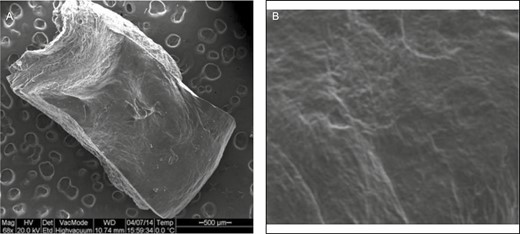
(A) Specimen obtained from the smooth surface of the intercapsular space of a double capsule as seen under scanning electron microscopy at 68× magnification. (B) Demonstration of the absence of bacteria under scanning electron microscopy at 400× magnification.
Therefore, the hypothesis that double capsule formation is caused by mechanical shearing stresses within the capsule itself through delamination of the collagen matrix is the only plausible explanation (Figure 3). This concept of intracapsular microfractures coalescing into delaminated layers of collagen matrix was previously described by Glicksman et al as part of their histological analysis of 8 specimens of double capsules.5 Our group also reported that not only was delamination present in all cases of partial double capsules, but the topographical location on the breast capsule played a central role.6 Indeed, all specimens from the lateral portion of the breast contained intracapsular microfractures and cracks, whereas none from the central dome of the breast did. Observing this delamination exclusively on the lateral border, where the junction of the tightly firm capsule adherent to the chest wall with the loosely mobile capsule of the anterior breast pocket occurs, further supports the hypothesis of a mechanical shearing etiology being responsible for double capsule formation.
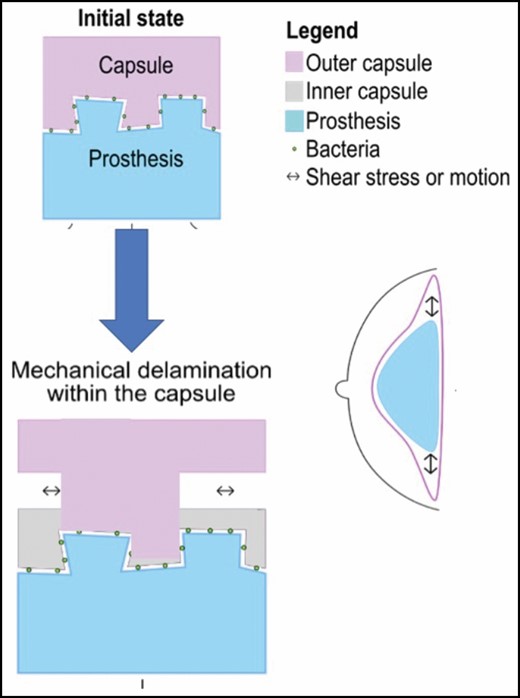
Illustration demonstrating the formation of double capsules by delamination at the border of breast implants of the native inner capsule which remains adherent to the prostheses by the “Velcro” effect.
Interestingly, Van Slyke et al found that 4 of the 6 specimens taken from the adherent portion of the capsule adjacent to partially formed double capsules demonstrated cracks histologically. We agree with the authors that adherent portions of the capsule onto the implant may be focal points of delamination which can lead to a cleavage plane of inner and outer layers in partial double capsules. However, is the nascent inner capsular layer, illustrated in Figure 2 of the original article, an event that occurs after nonadherence of the native capsule? In our opinion, based on our previous paper referenced above,6 it is more likely that the spectrum of nascent to well-formed inner capsules only represents different thicknesses of cleavage through delamination from external sheering forces. Furthermore, how can one explain physiologically that the avascular surface of an implant could be responsible for a nascent inner capsule if the outer native layer has already detached due to nonadherence?
Although one could debate that nonadherence is the inciting etiological event, we agree with the study’s senior author that Biocell implants seem to be associated with implant-related pain independent of capsular contracture. In this study, they reported that out of 6 patients who complained of painful implants, 2 demonstrated pain associated with areas of partial adherence. This novel idea brought up by the senior author merits further consideration, and we look forward to reading the findings of their unpublished work, which seem to indicate that these areas of pain coincide with partial adherence of capsules.
Although Biocell implants are now off the market, studies such as this one are important and we congratulate the authors on their work. Conditions such as breast implant–associated anaplastic large cell lymphoma and breast implant illness continue to gain awareness among the general public,7 which is why the clinical relevance of more readily understanding the phenomenon of double capsules can help the plastic surgeon in their practice when patients raise issues pertaining to implant-related pain. With increasing rates of explantation of macrotextured implants in the coming years, we firmly believe that incidental findings of double capsules will rise and we urge surgeons to collaborate in studies with larger cohorts to better understand and recognize this phenomenon.
Disclosures
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors received no financial support for the research, authorship, and publication of this article.
References


{kind=link}
{kind=link}
{kind=link}