



Abstract
Lercanidipine, a newer-generation calcium channel blocker, is recognized for its effective antihypertensive properties and reduced side effects. This study aims to compare the effectiveness of lercanidipine and amlodipine in preventing major adverse cardiovascular events (MACE) in hypertensive patients.
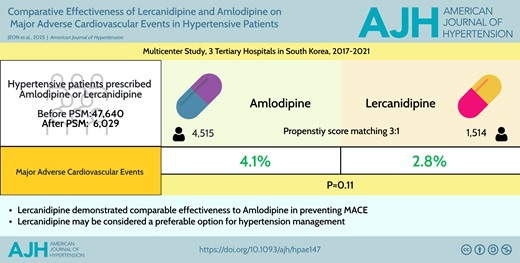
A multicenter, retrospective observational study was conducted using the electronic medical records database from 3 tertiary hospitals in South Korea between 2017 and 2021. Hypertensive patients treated with either amlodipine or lercanidipine were analyzed. Propensity score matching (PSM) was utilized to minimize confounders, matching patients in a 3:1 ratio. The primary endpoint was the incidence of MACE, a composite of cardiovascular death, myocardial infarction, stroke, heart failure hospitalizations, and coronary revascularization over a 3-year follow-up period.
A total of 47,640 patients were evaluated, and 6,029 patients were matched. Before PSM, the lercanidipine group had a higher cardiovascular risk (SCORE-2/SCORE-2OP value: 11.6% ± 9.2 vs. 10.9% ± 8.8, P < 0.01) and a higher incidence of MACE compared to the amlodipine group (4.1% vs. 3.4%, P < 0.01). After PSM, the incidence of MACE was numerically lower in the lercanidipine group compared to the amlodipine group (2.8% vs. 4.1%, P = 0.11), though this difference was not statistically significant. Blood pressure control remained comparable between the 2 groups over the 3-year follow-up period.
Lercanidipine demonstrated comparable effectiveness to amlodipine in preventing MACE among hypertensive patients. Given its comparable antihypertensive efficacy and potential for fewer side effects based on prior studies, lercanidipine may be considered a preferable option for hypertension management.



{kind=link}